Diabetes Type One and Type Two Showing Insulin Deficiency, Blood Sugar Levels, and Pancreas Function
Diabetes is a chronic metabolic condition rooted in the body’s inability to properly regulate blood glucose, the essential fuel that powers every cell and maintains energy balance. Although the word diabetes is often used broadly, two primary forms — Type 1 diabetes and Type 2 diabetes — differ significantly in their origin, insulin response, and progression inside the body. Understanding these differences through a conceptual illustration that highlights insulin production, pancreas function, and blood sugar dynamics helps reveal why the same symptom of high glucose levels can stem from two very different internal mechanisms. Both types disrupt the body’s sugar-regulating system, yet they do so in distinct ways: in one, insulin is nearly absent; in the other, insulin is present but cannot perform its job effectively. The result is the same on the surface — elevated blood sugar — but the biological stories leading there unfold on very different paths.
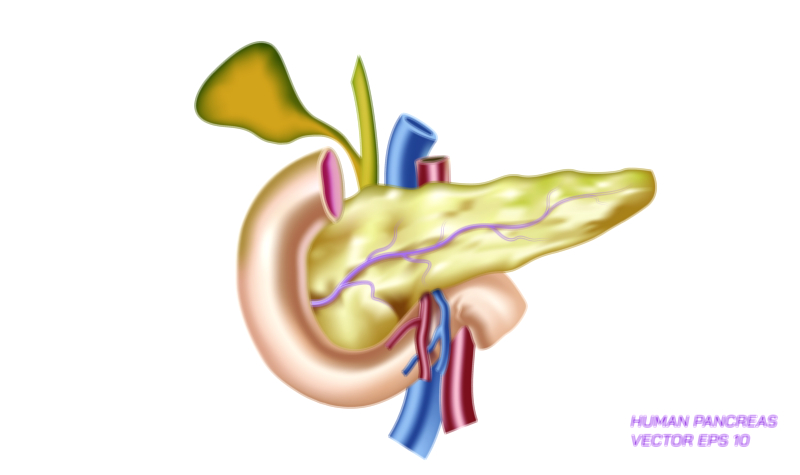
In a healthy individual, glucose enters the bloodstream after digestion and circulates for delivery to cells throughout the body. The pancreas, particularly the beta cells of the islets of Langerhans, closely monitors glucose concentration and releases insulin when levels rise. Insulin functions as the key that unlocks cells, allowing glucose to move inside where it can be converted to energy. Without insulin, or when insulin is unable to work effectively, glucose remains trapped in the bloodstream, slowly pushing blood sugar levels higher while cells go under-nourished. The pancreas–insulin–glucose relationship is at the heart of diabetes, and visual comparisons of Type 1 and Type 2 diabetes typically center around this triangular connection.
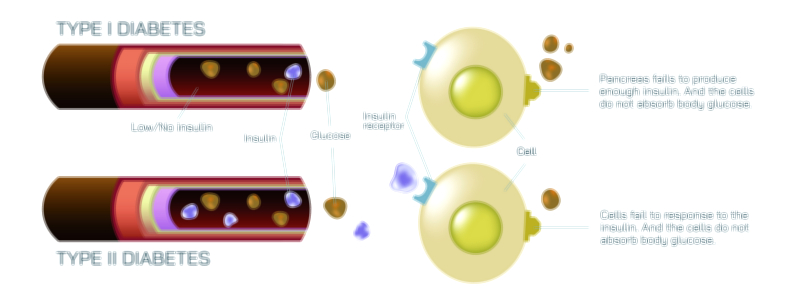
Type 1 diabetes is characterized by a near-total absence of insulin production. It develops when the immune system mistakenly targets and destroys the beta cells of the pancreas, eliminating the body’s ability to produce insulin. Because this destruction is typically rapid and severe, individuals with Type 1 diabetes rely on external insulin for survival. In illustration, Type 1 diabetes is represented by a pancreas releasing little to no insulin, along with arrows showing glucose remaining in the bloodstream because no biological key is available to open the door to the cells. Blood sugar rises sharply because glucose accumulates without a regulator, and energy balance inside the body is disrupted even though fuel is present but inaccessible. This autoimmune mechanism explains why Type 1 diabetes often appears in childhood or adolescence, though it can occur in adults as well. It also clarifies why people with Type 1 do not produce insulin naturally and cannot reverse their condition through diet or lifestyle; their pancreas no longer contains the cells that make insulin.
Type 2 diabetes, on the other hand, is rooted in insulin resistance, meaning insulin is present but cannot work properly. Early in the course of the disease, the pancreas still produces insulin — sometimes even more than usual — but cells no longer respond to it effectively. In illustration, Type 2 diabetes shows insulin being released by the pancreas, but arrows indicate that cells are no longer accepting glucose even though insulin attempts to open the doors. Because insulin cannot efficiently transport glucose inside the cells, the pancreas tries to compensate by producing even more insulin. Over many years, the pancreas becomes overworked and begins to lose its ability to keep up, leading to both insulin resistance and gradual insulin deficiency. Blood sugar levels rise steadily over time, not abruptly as in Type 1, and symptoms may remain unnoticed for years before diagnosis.
2. Both conditions produce hyperglycemia — high blood sugar — but through vastly different biological failures.
Symptoms also reflect these differences in timing and physiology. In Type 1, onset is rapid, often developing over days or weeks, leading to sudden weight loss, extreme thirst, frequent urination, irritability, fatigue, and in some cases, dangerous diabetic ketoacidosis. In Type 2, symptoms progress slowly and silently, with signs such as persistent thirst, tiredness, blurred vision, numbness, and slow wound healing gradually intensifying. Whereas Type 1 requires lifelong externally supplied insulin, Type 2 can be influenced by lifestyle and metabolic patterns. Exercise, nutrition, weight management, and medications that improve insulin sensitivity or reduce liver glucose production play major roles in treatment, though some individuals eventually require insulin when pancreatic function declines.
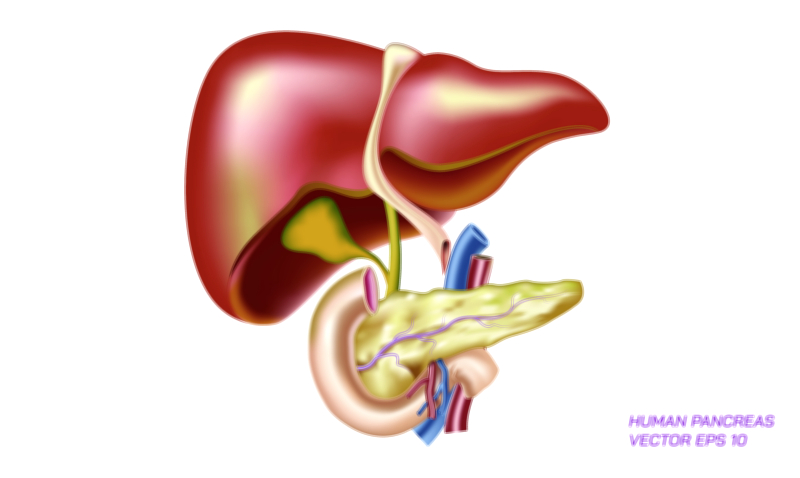
Yet beneath these differences, both types of diabetes converge at a deeper level — chronically elevated blood glucose harms tissues throughout the body when left unmanaged. Excess glucose gradually affects blood vessels, nerves, eyes, kidneys, and heart. Illustrations of unmanaged diabetes often show glucose molecules circulating persistently in the bloodstream, attaching to blood vessel walls and interfering with circulation. They also demonstrate the long-term effects on organs, reinforcing that regardless of the underlying cause, managing blood glucose is critical for preventing complications.
Another important link between both types is the metabolic struggle taking place at the cellular level. Cells deprived of glucose signal hunger even though the bloodstream is full of sugar. In Type 1, the hunger comes from absence of insulin; in Type 2, from resistance to insulin. This paradox — that the body can be overfilled with glucose yet starved for usable energy — explains fatigue and muscle weakness that people with diabetes experience. It also explains why the body begins to burn fat excessively in Type 1 when no insulin is available, leading to ketone buildup and potential ketoacidosis; in Type 2, insulin is present, so ketoacidosis is less common but can still occur in severe insulin deficiency later in the disease.
A full vector illustration comparing Type 1 and Type 2 diabetes typically includes:
• A pancreas graphic showing insulin absence in Type 1 and insulin production but resistance in Type 2
• Bloodstream glucose flow remaining outside cells in both types
• Cells illustrated as “locked” due to absent insulin in Type 1 or blocked receptors in Type 2
• Blood sugar level arrows rising in both conditions for different reasons
• Optional visual of insulin injection for Type 1 and lifestyle or medication support for Type 2
Seen through this visual and conceptual lens, diabetes becomes not simply a disorder of high blood sugar but a disease of disrupted communication between the pancreas, insulin, and cells. In Type 1, the message cannot be sent because insulin is missing. In Type 2, the message is sent repeatedly but ignored because the body has become resistant to hearing it. Yet both forms share the same ultimate goal in management: to restore balance so that glucose can move safely and efficiently into the cells where it belongs.
Understanding these differences deepens not only scientific insight but empathy. The challenges of diabetes are not merely numerical readings on a glucose meter but a constant negotiation between physiology, lifestyle, and self-care. Through the detailed depiction of insulin deficiency, resistance, pancreatic function, and blood sugar movement, the illustration of Type 1 and Type 2 diabetes brings clarity to a condition that millions of people navigate every day — a condition shaped by biology but anchored in the essential human need for energy, balance, and well-being.