Pancreas Ulcer and Cancer – A Comprehensive Medical Education Summary on Causes, Pathology, Cellular Damage, Symptoms, Diagnostic Challenges, Clinical Progression, Treatment Approaches, and the Life-Sustaining Role of the Pancreas in Human Health
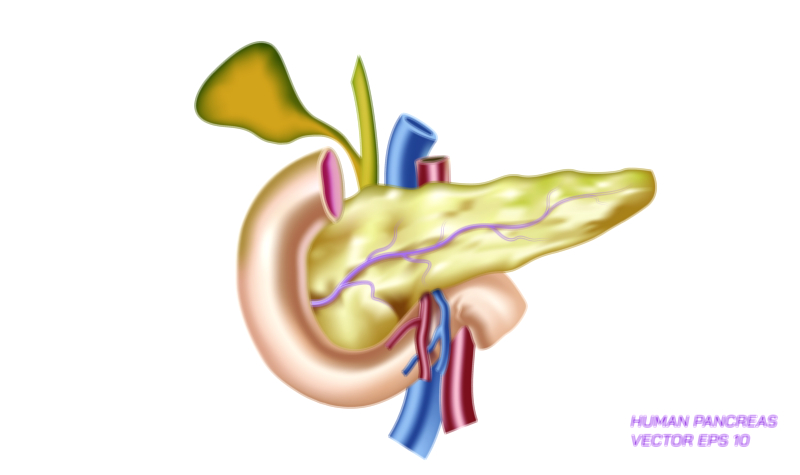
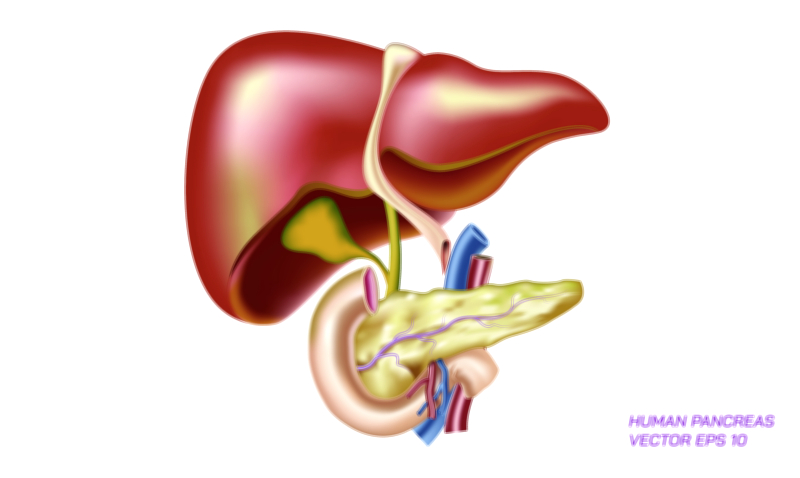
Pancreatic ulcer and pancreatic cancer represent two of the most serious and clinically challenging disorders affecting one of the body’s most vital organs, and although they are fundamentally different in origin, their symptoms and consequences reveal much about how essential the pancreas is to both digestion and metabolic regulation. The pancreas sits deep inside the upper abdomen, behind the stomach and close to the liver, small intestine, and major blood vessels. Because of its central position and its dual role—producing digestive enzymes through the exocrine component and controlling blood sugar through hormones such as insulin and glucagon from the endocrine islets—any structural injury or cellular disruption within the pancreas has the potential to influence the entire body. Pancreatic ulcers and pancreatic cancer, though distinct in mechanisms, highlight how inflammation, tissue destruction, genetic mutation, and metabolic imbalance can disrupt digestion, nutrient absorption, and energy availability. Understanding both conditions provides a deeper look into why pancreas-related illnesses often progress silently and severely before diagnosis, and why early medical attention, prevention, and awareness are crucial.
A pancreatic ulcer is a lesion that develops when the protective tissues of the pancreas become eroded, usually due to the abnormal backflow or premature activation of digestive juices, or due to chronic irritation and inflammation in the region where the pancreatic duct empties into the duodenum. Unlike stomach or duodenal ulcers, which are commonly caused by helicobacter pylori infection or excessive stomach acid, pancreatic ulcers are frequently secondary to other gastrointestinal disorders, such as chronic pancreatitis or duodenal ulcer extension into adjacent pancreatic tissue. In many cases, the underlying problem is persistent inflammation that weakens pancreatic tissue, or obstruction of the pancreatic duct that causes enzyme buildup inside the gland. When digestive enzymes activate prematurely inside the pancreas rather than inside the duodenum, they begin to digest pancreatic tissue itself. This self-destructive process causes extreme pain and cellular damage, and because the pancreas lies close to multiple organs, inflammation can radiate widely. Patients may experience severe upper abdominal pain that radiates to the back, nausea, vomiting, loss of appetite, unexplained weight loss, and intolerance to fatty meals because the pancreas can no longer release enzymes properly. As ulcers progress, digestive failure can occur due to reduced enzyme output, and blood glucose may become unstable if endocrine function is compromised, demonstrating how one localized lesion can trigger systemic consequences.
Pancreatic cancer, on the other hand, arises from mutations within pancreatic cells that drive uncontrolled growth rather than ulceration, and it is among the most aggressive and life-threatening cancers because of its silent development, deep anatomical location, and high capacity to spread early. Most pancreatic cancers develop from the exocrine cells responsible for enzyme secretion and take the form of adenocarcinomas originating in the ducts. Less commonly, cancers arise from the hormone-producing islets of Langerhans, creating neuroendocrine tumors that behave differently and have diverse hormonal effects. In the majority of cases, pancreatic cancer begins at the microscopic level through genetic and epigenetic changes that alter normal cell division, allowing damaged cells to survive instead of dying as they should. Risk factors include chronic pancreatitis, smoking, diabetes, obesity, hereditary mutations, family history, excessive alcohol use, and long-standing inflammation within the pancreas. Because early-stage pancreatic cancer rarely causes noticeable symptoms, tumors may grow silently while continuing to hijack metabolic resources. Once symptoms appear, the cancer has often grown large or spread to nearby organs and lymph nodes. Common warning signs include persistent abdominal or back pain, jaundice due to bile duct obstruction, loss of appetite, rapid weight loss, dark urine, pale stools, fatigue, and progressive malnutrition. Digestive problems intensify as the tumor interferes with pancreatic enzyme flow, and blood sugar may become unpredictable if insulin-producing cells are disrupted. These signs illustrate how pancreatic cancer disrupts both digestive and endocrine systems simultaneously.
Both pancreatic ulcers and pancreatic cancer underscore how vulnerable pancreatic tissue is to inflammation and pressure changes inside the duct system. In pancreatic ulcers, the immediate danger is tissue erosion and enzyme-driven destruction, while in pancreatic cancer it is unchecked abnormal cell multiplication. Yet both lead to pain, malabsorption of nutrients, weight loss, and metabolic instability because they hinder enzyme secretion and hormonal regulation. In both conditions, early diagnosis is difficult due to the pancreas’s deep anatomical position and because early symptoms can mimic common digestive problems. Imaging tests such as CT scans, MRI scans, MRCP studies, and endoscopic ultrasound are often necessary to evaluate pancreatic tissue properly. Blood tests can detect elevated pancreatic enzymes during ulcer-related inflammation or tumor markers such as CA 19-9 in some cancer patients, although these are not definitive alone. Endoscopic biopsy provides the final confirmation in suspected cancer cases. The difficulty of early detection contributes to the high risk and severity associated with pancreatic disease.
Treatment approaches diverge based on condition. Pancreatic ulcers are often managed with pain control, anti-inflammatory therapy, medications to reduce digestive acid secretion if duodenal factors are involved, control of pancreatitis triggers, infection treatment where necessary, lifestyle modification, and nutritional support. Severe ulcers that cause perforation or abscess formation may require surgical intervention. Pancreatic cancer treatment depends on tumor type, location, and stage. When discovered early enough, surgical removal of the tumor through procedures like the Whipple operation offers the best chance of survival, though only a minority of patients are eligible due to late diagnosis. Chemotherapy, radiation therapy, immunotherapy, and targeted molecular therapies are used alone or in combination to shrink tumors, slow progression, and relieve symptoms. Palliative care also becomes essential to manage pain, support nutrition, and maintain quality of life in advanced cancer. Despite advances in therapy, pancreatic cancer remains one of the most challenging malignancies in medicine because of its rapid spread and resistance to treatment.
The dietary and lifestyle dimension of pancreatic disease emphasizes prevention as much as treatment. Chronic alcohol consumption, high-fat diets, smoking, uncontrolled diabetes, and long-term inflammation increase the risk of both pancreatitis and cancer. Preventive strategies—limiting alcohol intake, maintaining a balanced diet, controlling blood sugar, avoiding tobacco, staying physically active, and treating digestive symptoms early—help preserve pancreatic health by reducing stress on the tissues and ducts. Awareness of symptoms such as persistent abdominal pain, rapid weight loss, jaundice, and digestive intolerance should prompt immediate medical evaluation rather than waiting. Recognizing risks early protects not only the pancreas but also the interconnected organs involved in digestion and metabolism.
In a broader medical context, pancreatic ulcer and pancreatic cancer demonstrate how a single organ can influence nearly every aspect of survival. When the pancreas fails, digestion falters, the body loses the ability to extract nourishment from food, and glucose control becomes erratic—leading to weakness, rapid weight changes, tissue damage, and vulnerability to infections. These conditions remind us that the pancreas is not a passive digestive gland but a central metabolic commander, constantly regulating energy and chemical balance. Studying pancreatic disease strengthens understanding of the interdependence of organs, the destructive power of inflammation and genetic mutation, and the importance of early medical attention for abdominal symptoms that might otherwise be overlooked. It teaches that protecting the pancreas is not only a matter of preventing pain, but of safeguarding digestion, blood sugar stability, energy supply, and the biochemical foundation of life itself.