All Types of Bone Fractures of the Femur Bone Showing Multiple Break Patterns and Healing Process
The femur, the strongest and longest bone of the human skeleton, is built to bear extraordinary pressure with every step, jump, and movement. Yet when exposed to forces beyond its structural capacity, the femur can break in a variety of distinct patterns, each reflecting the direction and magnitude of the impact and each requiring its own orthopedic strategy for stabilization and recovery. A detailed vector illustration showing all major types of femur fractures helps students, clinicians, and patients visualize how different mechanical forces create different break shapes, why some fractures remain stable while others shift dramatically, and how the body heals with the support of orthopedic treatment over time. Even though all fractures represent a loss of bone continuity, the pattern of the break determines both the severity of the injury and the complexity of the healing journey. When these patterns are placed side by side in a single educational illustration, the narrative becomes clearer: the femur does not simply break randomly — it fails in recognizable mechanical paths that mirror the forces applied to it.
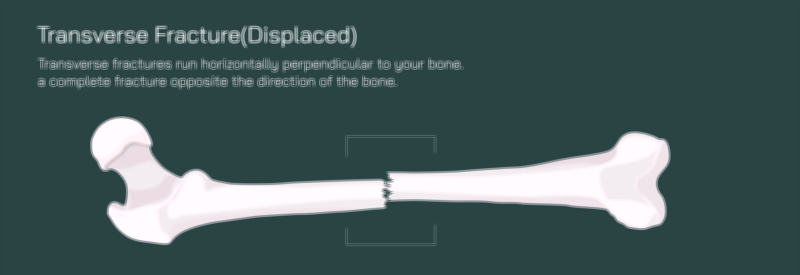
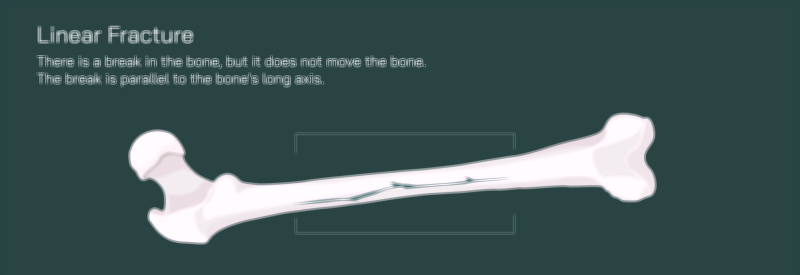
A transverse fracture represents one of the most straightforward patterns. In this injury, a force strikes the femur sideways, producing a clean horizontal break perpendicular to the bone’s long axis. If the fragments stay in place, the fracture is stable; if they shift apart, it becomes displaced, often creating limb shortening or deformity. A linear fracture, in contrast, forms a lengthwise crack parallel to the femur’s shaft, usually without separation. It is a quieter injury, sometimes missed initially because the bone remains aligned while pain intensifies during weight-bearing. A hairline fracture presents an even subtler version: a thin crack caused by repetitive stress that does not extend completely through the bone, yet compromises structural integrity and risks progression if not treated early.
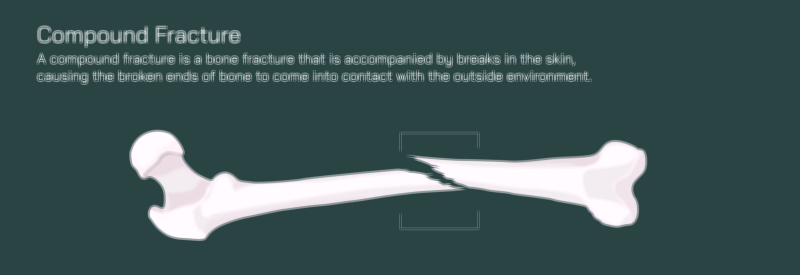
The opposite extreme occurs in a comminuted fracture, where the femur shatters into three or more fragments — the dramatic result of high-energy trauma such as vehicle collisions or falls from height. Because multiple irregular fragments cannot realign naturally, orthopedic stabilization becomes complex and urgent. A compound fracture, also called an open fracture, is not defined by the break shape itself but by the fact that bone pierces the skin, exposing the fracture to the external environment. Compound fractures can accompany transverse, oblique, spiral, or comminuted patterns but add the severe complication of infection risk and soft-tissue damage.
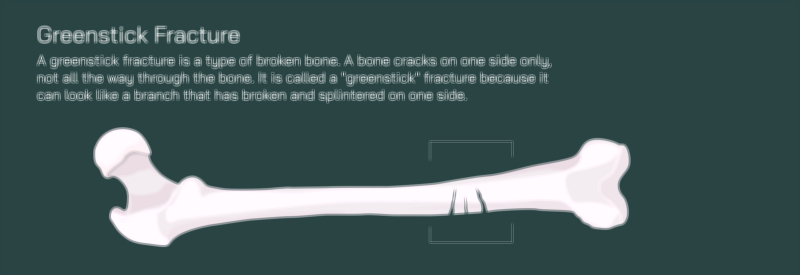
Some fracture shapes reflect the direction of mechanical twisting rather than direct impact. A spiral fracture winds around the bone in a corkscrew pattern caused by rotational force, while an oblique fracture forms a clean diagonal line that results from angled compression. Both patterns are unstable because muscle contractions tend to slide fragments across their slanted surfaces, making realignment and stabilization essential for healing. In children, the still-developing skeleton gives rise to distinct patterns not seen in adults. A greenstick fracture involves bending of the bone with cracking of only one side, leaving the opposite cortex intact but deformed; this partial break requires realignment to keep the bone from healing with curvature. A buckle or torus fracture, another pediatric pattern, does not produce a crack but instead compresses the outer layer of the bone inward, usually from axial loading during falls. Each of these can be represented in a vector illustration with characteristic shapes that immediately identify the mechanics of injury.
Despite their different appearances, all femur fractures trigger the same biological sequence of repair once alignment and stability are achieved. Healing begins with the inflammatory phase, when blood surrounds the break to form a hematoma that attracts immune cells and repair factors. This early stage clears debris and prepares the fracture for reconstruction. During the soft callus phase, connective tissue and fibrocartilage begin bridging the fractured areas — whether it is a single clean line or a cluster of fragments — creating an internal biological brace. Over the weeks that follow, the hard callus phase begins as minerals such as calcium and phosphorus accumulate within the soft callus, turning it into hardened bone strong enough to tolerate controlled loading. Finally, the remodeling phase reshapes this new bone and restores its original architecture, smoothing excess callus and reorganizing internal structure according to stress patterns imposed by movement and weight-bearing. A vector timeline showing a femur progressing from fracture through callus formation to complete restoration allows viewers to see that healing is complex, gradual, and dependent on proper alignment.
The orthopedic interventions required for stabilization vary dramatically depending on the fracture type. Stable fractures like isolated linear or nondisplaced transverse cracks may heal with immobilization, crutches, and activity restriction alone. Most femur fractures, however, require internal fixation, most commonly through intramedullary nailing, in which a metal rod is inserted through the marrow canal and locked with screws. Other fractures, particularly oblique, comminuted, or fractures near joints, may require plates and screws to hold fragments firmly against one another. Severe injuries involving soft-tissue trauma may be temporarily managed with external fixation, where pins anchored through the skin are connected to an external frame to maintain limb alignment until internal repair becomes safe. When pediatric greenstick or buckle fractures are present, immobilization through casting or bracing is often enough because children’s bones heal rapidly and remodel naturally when alignment is correct.
Once stabilization is achieved, rehabilitation becomes as important as the fracture repair itself. The femur is central to mobility, and long periods of reduced movement cause thigh muscles — quadriceps, hamstrings, and gluteals — to weaken quickly. Physical therapy restores joint mobility at the hip and knee, retrains gait, rebuilds strength, and prevents stiffness or muscle imbalance. A vector illustration outlining the progression from non-weight-bearing to partial weight-bearing and eventually to full ambulation helps communicate that rehabilitation evolves step by step, centered around imaging confirmation of healing and patient comfort.
Nutrition and metabolic balance reinforce the healing timeline. Adequate calcium supports mineralization of the hard callus; vitamin D improves absorption and delivery of calcium; magnesium stabilizes bone chemistry; protein drives collagen production; and hydration supports cellular repair. In older adults, individuals with osteoporosis, or patients with repeated fractures, medical management of bone density may accompany orthopedic treatment. These physiological interactions are often rendered visually by placing nutrient symbols around the healing bone in the illustration.
Complications arise when fractures heal improperly. If alignment is not achieved or maintained — especially in displaced transverse, spiral, or oblique fractures — malunion can occur, leaving the leg rotated, shortened, or bowed. In cases where healing does not progress, nonunion or delayed union may develop, requiring additional surgery or bone stimulation. Complex comminuted or compound fractures have added risks, including infection, persistent pain, and joint strain. An educational graphic showing the difference between a successfully aligned healing femur and a malaligned bone makes the value of proper orthopedic management immediately clear.
In its deepest educational role, a vector illustration showing all major types of femur fractures and the healing process tells a story of mechanical failure and biological restoration. It allows the viewer to compare fracture patterns side by side, understand why each injury requires a different treatment strategy, and see how the body — with orthopedic support — rebuilds bone tissue until strength returns. It offers clarity for medical learners trying to differentiate fracture types, reassurance for patients trying to visualize their recovery, and insight for families supporting rehabilitation. Most importantly, it shows that while fractures vary in shape, severity, and treatment pathway, the combination of precise alignment, stability, nutrition, and time enables the femur to return to its essential role in supporting posture, movement, and lifelong mobility.