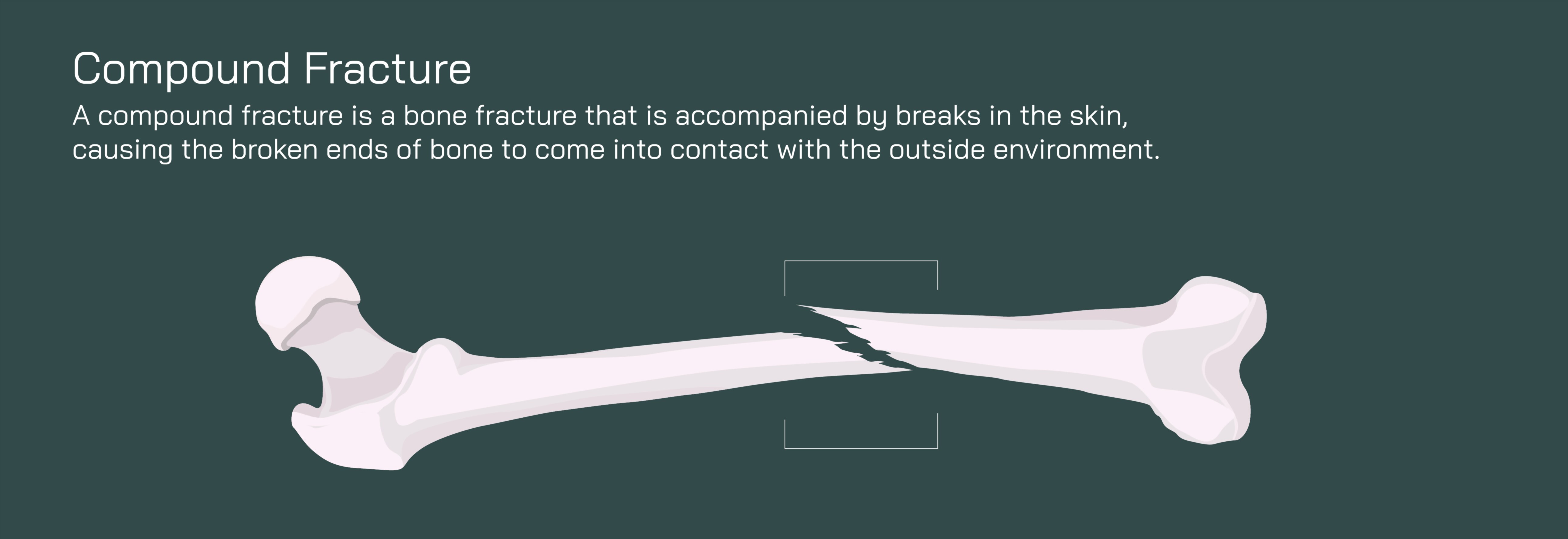
Compound Fracture of the Femur Bone Showing Open Break and Orthopedic Treatment
A compound fracture of the femur is one of the most severe and traumatic injuries that can occur within the skeletal system, and a medical or educational vector illustration showing an open break in the femur and the orthopedic treatment process provides an essential visual explanation of both the damage and the long road to recovery. Unlike closed fractures, where the broken femur remains contained beneath the skin, a compound fracture pierces through the surrounding soft tissues and breaks the skin surface, exposing the fractured bone to the outside environment. This exposure drastically increases the risk of deep infection, heavy bleeding, and long-term disability if not treated immediately and appropriately. Even though the femur is anatomically the strongest and thickest bone in the human body, capable of supporting immense load and stress during walking, running, and jumping, traumatic forces such as vehicle collisions, falls from significant heights, or industrial accidents can overwhelm its structural integrity. Vector illustrations depicting this injury typically show a clearly displaced break in the shaft of the femur, the protrusion of one or both bone fragments outside the skin, torn muscle fibers around the break, disrupted blood vessels, and acute swelling — all of which communicate the urgency and seriousness of the injury in a way that simple text alone cannot.
A compound fracture of the femur is not only a skeletal emergency but a soft tissue and systemic emergency. When the bone punctures the skin, it drags bacteria and debris from the surrounding environment deep into the wound, creating a direct pathway for infection to enter the bone marrow and bloodstream. Because the femur contains an extremely rich vascular supply, bleeding can be substantial, and if blood loss is severe, shock may develop rapidly. An illustration that highlights ruptured vessels and leaking blood can help explain why uncontrolled bleeding at the scene of the accident is a critical threat and why paramedic stabilization — such as applying dressings, splinting the leg, and preventing further movement — is life-saving. The break also causes extreme disruption to the surrounding muscles, ligaments, periosteum, and nerves, and the leg often appears shortened, rotated outward, or otherwise deformed due to the strong pull of thigh muscles on the separated bone fragments. Showing the direction of muscle tension and limb deformation graphically enables students and caregivers to understand how the forces of the body itself can worsen the displacement.
Emergency care begins with infection control, bleeding management, pain reduction, and limb stabilization. The open wound must be irrigated and cleaned thoroughly, often removing dirt, dead tissue, and foreign material brought into the body at the time of injury. Broad-spectrum intravenous antibiotics are started immediately to reduce the risk of bone infection (osteomyelitis). A vector depiction might show a stepwise sequence beginning with wound cleaning, temporary wound coverage, and splinting of the affected leg to prevent further tissue tearing. In high-energy injuries, the damage often affects not only bone but the overlying skin and deep fascia. When illustrated, these torn structures visually underscore why orthopedic surgeons must evaluate not only the fracture but the entire soft-tissue envelope before definitive repair.
The orthopedic treatment of a compound femur fracture nearly always requires surgical intervention because the bone fragments must be realigned and stabilized securely to heal. Surgery typically begins with debridement — the surgical removal of infected or non-viable tissue — followed by irrigation of the wound to flush out contaminants. Once the fracture site is clean and prepared, realignment of the femur is achieved. Graphically, this is often shown as bringing the displaced fragments together into correct alignment with the help of traction or manipulation. After repositioning the fragments, internal fixation is performed to hold the bone in place while healing occurs. The most common treatment is intramedullary nailing, in which a long metal rod is inserted down the center of the femur and secured with locking screws at both ends. This technique provides strong internal support and allows early, controlled weight-bearing in many cases. A vector illustration of this hardware — showing the nail within the marrow canal and screws securing the rod to the bone — makes the mechanics of fracture stabilization clear.
In cases where the bone is shattered into multiple fragments, where the skin and soft tissues are severely damaged, or where the wound is excessively contaminated, external fixation may be used first. This method attaches metal pins into the bone above and below the fracture site and connects them externally with metal bars, holding the femur in alignment while the wound heals and infection risk decreases. A graphic of external fixation visually distinguishes it from internal fixation by showing stabilizing hardware outside the body. Later, when soft-tissue healing is sufficient, a second surgery may convert external fixation to internal fixation for long-term stability. In especially complex fractures, plates and screws may be required to secure bone fragments, and bone grafting may be necessary to replace tissue lost during trauma.
Healing from a compound femur fracture is slow because the injury affects both bone and soft tissue. The healing timeline follows the biological remodeling process: blood clot formation at the fracture edges, soft callus formation, hard bony callus formation, and final remodeling over many months. A vector representation of this timeline reinforces that even with hardware in place, the body must still repair the bone itself, gradually reconnecting and strengthening the fracture through mineralization and reshaping. Because the bone has experienced extreme trauma, the risk of complications remains high, including delayed union, nonunion, infection, and deep tissue scarring. This is why post-operative management includes continued antibiotics when necessary, wound monitoring, physical therapy, weight-bearing progression under medical supervision, and long-term follow-up imaging.
Rehabilitation is critical not only for bone healing but for restoring strength, mobility, and gait mechanics. The muscles around the femur — quadriceps, hamstrings, gluteals, and adductors — often weaken dramatically during immobilization. Physical therapy re-educates these muscles while teaching safe movement and preventing stiffness in the hip and knee. A vector illustration of the rehabilitation stage might depict repetitive motion exercises, progressive loading, crutch-to-cane transition, and eventually full ambulation. Even once the fracture has healed radiographically, the bone continues strengthening for many months, and premature return to high-impact activity risks hardware failure or re-fracture. The illustration of a fully healed femur, with uniform cortical thickness around the remodeled fracture site, effectively communicates the goal of treatment and the payoff of patience.
A compound femur fracture is a life-changing event for many individuals, but with prompt care, effective orthopedic repair, infection control, rehabilitation, and proper nutrition, full recovery and return to activity are possible for the majority of patients. Visually showing the injury — the open break, exposed bone, displaced fragments, and torn tissue — alongside the surgical repair and the natural healing sequence allows patients, families, students, and clinicians to grasp the seriousness of the condition while appreciating the sophistication and effectiveness of treatment. It makes clear that bones are not simply rigid structures that break cleanly and heal automatically; they are biologically active organs that require precision care, time, and strategic support to restore strength and function.
A compound fracture of the femur is therefore not just a break — it is a medical emergency that demands an orchestrated response blending immediate first aid, orthopedic surgery, infection prevention, pain management, and structured rehabilitation. A detailed vector illustration captures this reality in one cohesive visual narrative: the trauma, the disruption of anatomy, the urgency of intervention, the reconstruction through fixation, and the long but transformative process of healing back toward normal mobility.