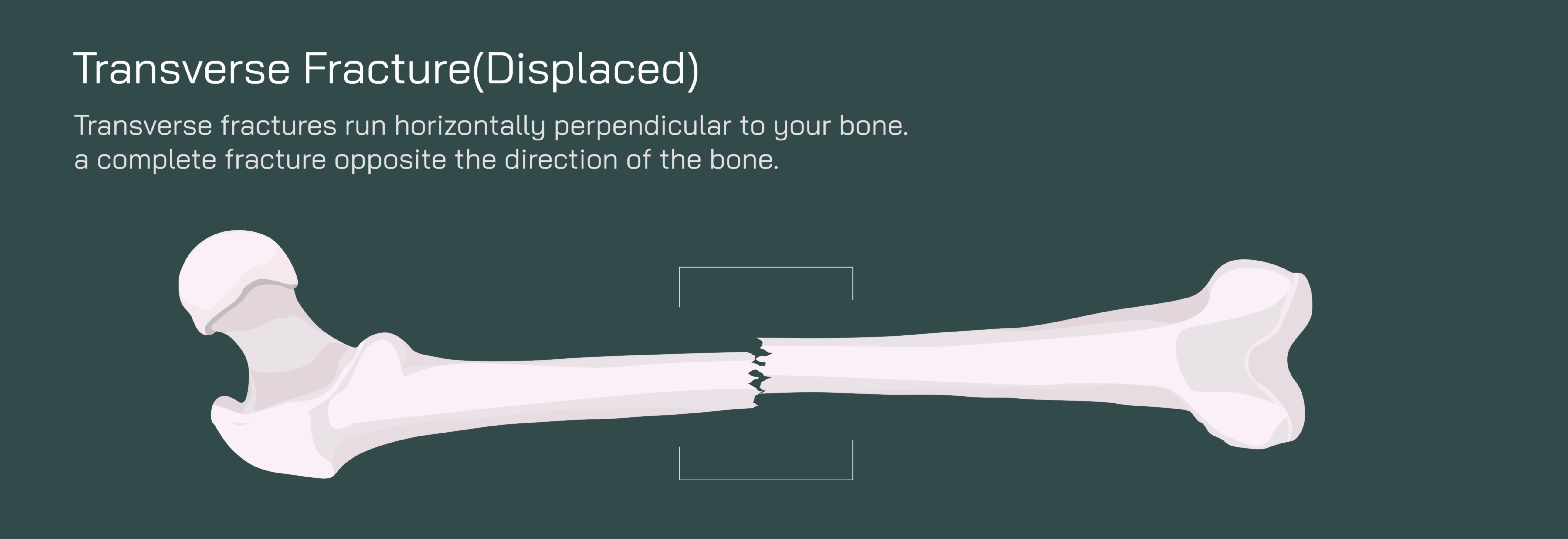
Transverse Fracture of a Displaced Bone Showing Horizontal Break and Orthopedic Realignment Process
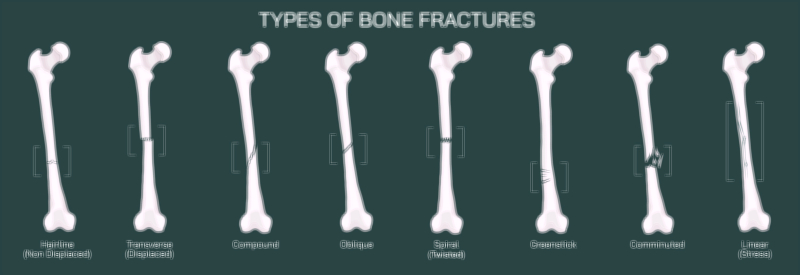
A transverse fracture is one of the clearest and most sharply defined fracture patterns seen in long bones, characterized by a horizontal break perpendicular to the long axis of the bone. Unlike spiral, oblique, or comminuted fractures — which involve diagonal, twisting, or fragmented patterns — a transverse fracture presents as a straight, clean line that runs directly across the shaft. When this type of fracture is displaced, the two bone fragments not only fracture across a horizontal plane but also shift apart, no longer maintaining their normal anatomical alignment. In a vector illustration, this injury is depicted as a complete horizontal separation with one bone segment shifted upward, downward, or sideways relative to the other — clearly showing that continuity has been lost. The visual emphasizes the full structural failure of the bone and the need for orthopedic intervention to restore alignment and prevent long-term complications.
The mechanical cause of a transverse fracture is typically direct force applied perpendicular to the bone’s length, such as a blow to the thigh during a fall, collision during a sport, a vehicular accident, or a forceful impact from a heavy object. Because the femur, tibia, humerus, or other long bones are built to withstand compression along their axis, a direct side-to-side impact overloads the bone in a mechanically vulnerable direction, producing the distinct horizontal break. In displaced cases, muscle contractions often worsen the separation. Long bones are surrounded by powerful muscle groups — quadriceps and hamstrings in the thigh, deltoids and rotator cuff in the upper arm — and once the bone loses integrity, the tension from these muscles can pull fragments apart. A vector depiction showing muscle forces acting on the broken bone helps explain why the fragments shift further after the initial break and why immediate stabilization is necessary.
Clinical presentation is dramatic: sudden sharp pain at the fracture site, rapid swelling and bruising, inability to bear weight or move the affected limb normally, and obvious deformity when the displacement is visible externally. The leg or arm may appear shortened, rotated, or bent due to the misaligned fragments. In contrast to hairline or stable fractures, a displaced transverse fracture causes complete loss of structural support, which is why patients cannot use the affected limb without severe pain or risk of further damage. Imaging — especially X-rays — confirms the diagnosis, typically showing a crisp horizontal fracture gap and misaligned bone edges. Illustrations that overlay a normal femur next to a transverse displaced fracture highlight how efficiently medical imaging identifies separation and loss of anatomical continuity.
Because of complete separation, orthopedic realignment is mandatory. The primary objective of treatment is to return the bone fragments to their original position — a step known as reduction — and then stabilize them long enough to allow the body to rebuild bone across the fracture line. Reduction may be performed through closed reduction, in which the orthopedic surgeon manipulates the bone externally without an incision, or open reduction, in which surgery is required to visualise and realign fragments directly. A vector diagram showing before-and-after alignment helps patients and learners immediately understand the function of reduction — the fragments must be placed back together precisely for healing to occur correctly.
Once realignment is achieved, the fragments must be kept immobile to prevent re-displacement. The most common and most effective stabilization technique for transverse fractures of major long bones is internal fixation, particularly:
• Intramedullary nailing — a metal rod inserted through the central marrow canal and secured with locking screws above and below the fracture site.
• Plates and screws — when the fracture is near a joint, when internal nailing is not appropriate, or when fragment control requires direct surface fixation.
• External fixation — used when soft-tissue damage or swelling prevents internal fixation initially; stabilizing rods and pins remain outside the body to hold bone segments in place.
A vector illustration showing hardware bridging the horizontal fracture line helps clarify how orthopedic fixation neutralizes shear forces and prevents fragments from sliding. Without stabilization, weight-bearing or muscle contraction could reopen the fracture repeatedly, preventing healing and risking long-term disability.
Once the fracture is realigned and stabilized, the body initiates its biological healing response. A transverse fracture — though severe — typically heals with predictable bone regeneration when alignment is correct. The healing timeline involves four interdependent phases:
Inflammatory Phase (immediate to first days): A hematoma forms around the break; immune cells clear damaged tissue and signal bone-forming cells to activate.
Soft Callus Phase (weeks 2–6): New tissue — collagen and fibrocartilage — begins bridging the horizontal fracture gap. Although not strong enough for full weight-bearing, the fragments become biologically connected.
Hard Callus Phase (weeks 6–12): Calcium and phosphorus harden the soft callus into new bone, restoring structural support and allowing greater mechanical loading.
Remodeling Phase (months to years): The bone adapts to stress and gradually reforms into its original cylindrical shape, strengthening itself according to weight-bearing patterns.
Vector diagrams showing progressive filling of the fracture gap with callus, followed by reshaping of the bone cortex, enable viewers to visualize how internal repair takes place long after external symptoms begin to fade.
Rehabilitation plays a major role in the alignment-dependent healing process. While the bone regains structural strength internally, muscles, tendons, and joints must be retrained to restore mobility and prevent long-term stiffness or gait abnormalities. Physical therapy usually includes:
• Protected weight-bearing that increases gradually as healing progresses
• Strengthening of surrounding muscle groups to restore joint function
• Stretching to regain range of motion
• Gait training to normalize walking patterns
A vector illustration showing the transition from immobilization to assisted walking and finally independent activity underscores that healing is progressive and guided.
Nutrition and systemic health reinforce orthopedic repair. Adequate calcium, vitamin D, magnesium, protein, and hydration support mineralization and collagen synthesis. Smokers, individuals with osteoporosis, or patients with chronic illness may require additional medical support to optimize healing and prevent delayed union or nonunion.
If alignment is not corrected or maintained, complications can include:
• Malunion (bone heals in the wrong position)
• Nonunion (bone fails to heal)
• Limb length discrepancy
• Chronic pain or altered gait mechanics
Vector comparisons of properly aligned healing versus malaligned healing communicate why strict adherence to orthopedic follow-ups and rehabilitation instructions is essential.
In its full educational purpose, a vector illustration of a transverse displaced fracture showing a horizontal break and orthopedic realignment process does more than display a broken bone — it visually narrates the entire path from injury to recovery. It shows how a perpendicular force breaks the bone, how displacement disrupts structural function, how surgeons restore anatomical alignment, how internal stabilization allows the body to regenerate bone, and how rehabilitation returns strength and mobility. For medical learners, orthopedic specialists, physical therapists, patients, and families, such a visual tool transforms an internal, complex healing process into an understandable and empowering story — demonstrating that while bone trauma can be severe, precise treatment and biological resilience work together to restore motion, stability, and full skeletal function.