Linear Fracture of the Femur Bone Showing Straight Crack and Orthopedic Healing Process
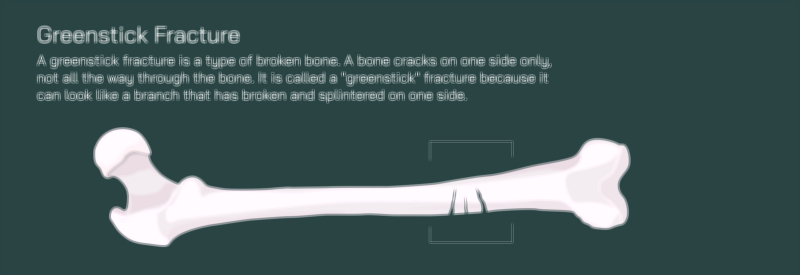
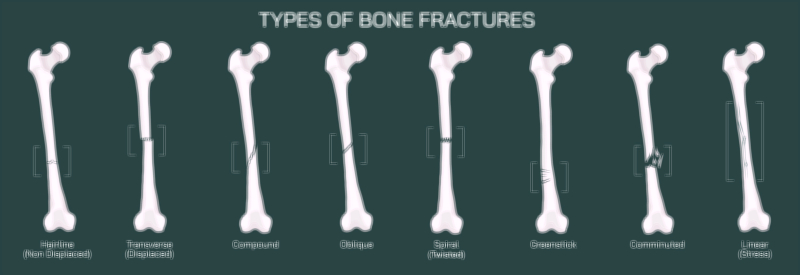
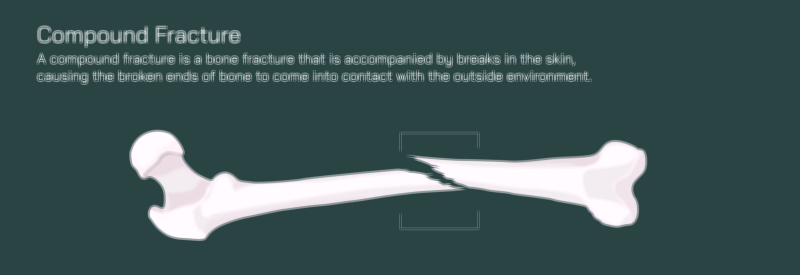
A linear fracture of the femur is a significant skeletal injury characterized by a straight, lengthwise crack along the bone without displacement of fragments, meaning the bone remains properly aligned but has suffered a structural failure along one side or across its shaft. Unlike comminuted, spiral, or greenstick fractures, a linear fracture does not split the bone into multiple pieces or cause rotation or bending of the shaft. Instead, the crack travels in a straight path—often parallel to the bone’s long axis—creating a thin but serious break that compromises the femur’s ability to bear weight safely. In a vector illustration, this injury is typically depicted as a narrow, clean line along the femoral shaft, showing that the outer cortical layer has fractured but the bone has retained its shape. Since the femur is the largest and strongest bone of the body, capable of supporting immense compressive and shear forces, a linear crack implies substantial trauma such as falls, sports injuries, automobile collisions, high-impact landings, or sudden loading forces. Even in the absence of visible deformity, a linear femur fracture demands rapid diagnosis and treatment because continued stress can convert the straight crack into a complete break.
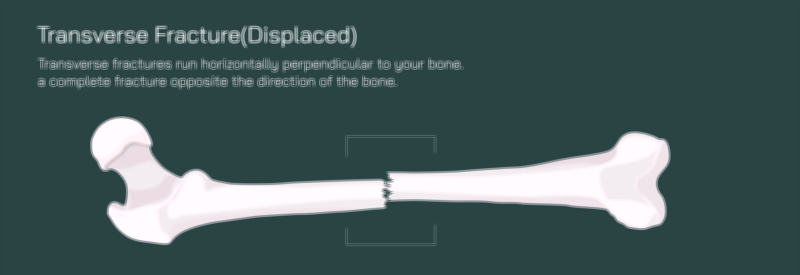
The visual significance of a linear femoral fracture lies in how deceptively stable it may appear from the outside. There is no bending or shortening of the leg, unlike displaced fractures, and swelling may be moderate rather than dramatic. Patients often experience sharp localized pain in the thigh, especially during standing, walking, or rotation of the leg. Reflex tightening of the quadriceps and hamstring muscles—part of the body’s natural protective mechanism—can intensify discomfort. In children, teenagers, and adults alike, pain can range from mild to severe depending on crack depth, the extent of cortical compromise, and overall bone density. An illustration that positions the crack line along the femoral shaft while keeping the bone’s linear shape intact helps distinguish linear fractures from other complex patterns and conveys why clinical symptoms rather than outward deformity guide diagnosis.
Imaging—typically X-ray followed by CT in uncertain cases—confirms the diagnosis. Radiographs show a sharply defined line through the dense cortical layer of the femur, with no separation of bone ends. A vector depiction may contrast healthy cortical bone on one side with the straight fracture line on the other to highlight how even a small crack damages structural integrity. Because linear fractures often follow the long axis of the femur, they allow viewers to appreciate the direction of applied force—usually compressive or impact-based. In some cases the crack may cross into trabecular bone, and illustrations showing both cortical and inner bone involvement help explain how pain and healing requirements increase with fracture depth.
Although linear fractures do not involve fragment displacement, orthopedic treatment is still required to prevent worsening, ensure healing, and protect mobility. The primary goal of management is to keep the crack from propagating further. If the fracture extends even a few millimeters under continued stress, weight-bearing forces can split the femur fully and produce a displaced or comminuted fracture requiring major surgery. For this reason, stabilization and load control form the cornerstone of treatment. Many linear fractures can be managed non-surgically if they remain stable. Orthopedic care usually begins with rest and restricted weight-bearing using crutches or walkers to avoid placing pressure on the healing bone. A rigid brace, long-leg cast, or functional support device may be used to limit rotation and maintain alignment. A vector illustration showing the femur within a brace alongside the fracture site conveys why immobilization prevents crack expansion.
In certain cases—particularly when the fracture line is long, extends into the hip or knee region, or occurs in bones that are already weakened—surgical stabilization may be recommended. This is often achieved with intramedullary nailing (a metal rod placed through the marrow canal), plates and screws along the bone surface, or occasional use of external fixation in high-risk trauma cases. A vector graphic that places hardware over the linear crack helps viewers see how internal support prevents stress along the fracture line and allows safe mobilization.
Healing of a linear femur fracture follows the traditional biological process of bone repair, and illustrations showing each stage make the timeline easier to understand:
• Inflammatory Phase (first days) — Blood forms a hematoma at the crack site, triggering cellular cleanup and preparation for tissue repair.
• Soft Callus Phase (weeks 2–6) — Collagen and cartilage fill the crack region, producing a cushioning bridge that stabilizes the fracture internally.
• Hard Callus Phase (weeks 6–12) — Calcium and phosphorus mineralize the soft callus, creating solid new bone that gradually replaces the fracture line.
• Remodeling Phase (months to years) — Newly formed bone reshapes and thickens, restoring original strength and structure.
A vector illustration that tracks this sequence—from the initial straight crack to progressive callus build-up and final bone remodeling—effectively conveys how healing is gradual, internal, and biologically complex even when the fracture does not involve deformation.
Rehabilitation begins once pain decreases and early healing is confirmed on imaging. Weight-bearing is gradually increased under orthopedic guidance, helping stimulate mineral deposition and bone density restoration. Physical therapy focuses on improving hip and knee mobility, rebuilding quadriceps and hamstring strength, correcting gait alterations, and preventing long-term stiffness. An educational graphic showing progression from crutches to normal walking helps patients understand why recovery is phased rather than immediate.
Nutrition and systemic health also play meaningful roles. Adequate intake of calcium, vitamin D, magnesium, and protein supports bone mineralization and collagen synthesis during callus formation. In older adults or individuals with low bone density, supplemental treatment may be necessary to avoid delayed healing or risk of refracture. If returning to sports or strenuous physical activity too early, the original straight crack can reopen, which is why visual guidance on safe return-to-activity timelines is helpful in educational illustrations.
Although linear femur fractures generally heal well when managed properly, untreated or prematurely stressed injuries can progress to more serious states including nonunion, malunion, complete fracture with displacement, chronic pain, or gait abnormalities. A comparison image showing a fully healed femur versus a crack that worsens due to early overloading reinforces the importance of compliance with orthopedic recommendations.
By showing the straight crack pattern, stabilization methods, stages of biological healing, and rehabilitation milestones, a vector illustration of a linear femur fracture becomes a comprehensive guide for clinicians, students, patients, and families. It makes clear that even without dramatic deformity, a linear fracture represents a real break that requires time, protection, and metabolic support to restore full bone strength. It transforms the invisible healing science occurring inside the femur into a visible, understandable narrative—one that reminds us that bone recovery is a delicate partnership between medical care, biology, and patient cooperation, ultimately returning the femur to its crucial role in weight-bearing, movement, and lifelong mobility.