Comminuted Fracture of the Femur Bone Showing Multiple Fragments and Orthopedic Healing
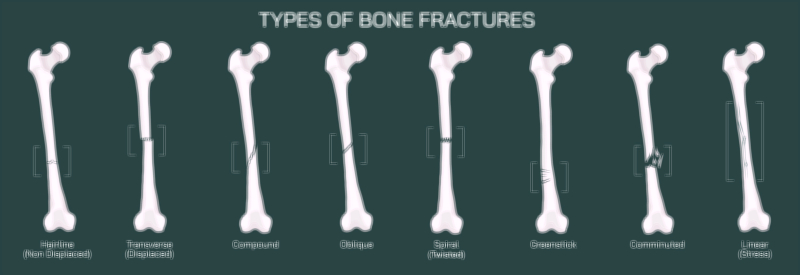
A comminuted fracture of the femur is among the most complex and mechanically devastating injuries that can occur within the skeletal system. In this type of fracture, the femur does not simply crack or split into two pieces — instead, the bone shatters into three or more fragments, often producing irregular edges and displaced pieces that cannot realign naturally. A vector illustration depicting this injury typically shows the femoral shaft broken into multiple fragments of varying shapes and sizes, with jagged bone edges and interrupted cortical continuity. Because the femur is the body’s main weight-bearing bone, its fragmentation represents an enormous disruption in structural stability, immediately compromising mobility and posing a serious risk to surrounding muscles, vessels, and nerves. High-energy trauma such as motor vehicle collisions, falls from height, industrial accidents, or significant blunt force impact is usually required to generate this degree of bone destruction.
The internal consequences of a comminuted fracture extend far beyond the shattered bone surfaces. When the femur breaks into multiple fragments, the surrounding muscular envelope — including the quadriceps, hamstrings, and adductors — is typically torn or violently stretched. These powerful muscles pull unevenly on the bone pieces, worsening displacement and misalignment. Bleeding is often severe, due to the femur’s rich vascular supply and sharp bone fragments cutting through soft tissue. Swelling, bruising, and extreme pain are immediate, and the deformity of the leg is often visible externally, sometimes presenting as shortening or rotation of the limb. A vector illustration that highlights displacement forces and scattered fragments helps convey why this injury cannot heal without surgical intervention.
Orthopedic healing for a comminuted femur fracture is designed to do three critical things simultaneously: realign the bone fragments, stabilize them rigidly, and preserve blood supply to the fracture zones. Unlike simpler fractures that may heal with a cast, the complexity and instability of a comminuted fracture make internal fixation the standard of care. Surgical treatment usually begins with an imaging-guided evaluation of every fragment, sometimes using CT scans to map fragment patterns. After fractures are identified, orthopedic surgeons must reposition the bone pieces as closely as possible to their anatomical alignment. This step — known as reduction — is one of the most technically challenging aspects of treatment, because restoring the femur’s length, rotation, and alignment is necessary both for structural support and for normal gait mechanics.
The most common stabilization method for comminuted femur fractures is intramedullary nailing, in which a strong metal rod is inserted down the marrow canal of the femur and secured using locking screws above and below the fracture region. A vector illustration that shows the nail running through the bone, with screws anchoring its upper and lower ends, helps viewers see how this internal framework keeps all fragments aligned while the bone heals. In some cases, plates and screws may be applied along the exterior surface of the bone to secure smaller fragments or reinforce the primary fixation. For extremely severe fragmentation or soft-tissue injury, external fixation may be used temporarily, with metal pins placed through the skin into the bone and connected to an external frame until internal fixation becomes safe. Illustrating differences between external and internal stabilization makes the treatment pathway clearer for students and patients.
Healing of a comminuted fracture relies on the body’s natural multi-stage repair cycle, but because the bone is shattered in multiple places, this process tends to be slower and more vulnerable to complications. The healing timeline can be broken into four continuous biological phases:
Inflammatory Phase — Immediately after injury, blood collects around the fragments, forming a hematoma that attracts immune cells and bone-building precursor cells. An illustration may show this as a darkened area around the fracture.
Soft Callus Phase — Over the following weeks, collagen and cartilage begin bridging the fragments. With a comminuted fracture, these bridges must extend to multiple bone fragments at once, and flexibility remains limited. A vector representation often shows the early callus as a soft, cloudy connection around the fragment cluster.
Hard Callus Phase — Minerals including calcium and phosphorus transform the soft callus into a hard bony callus. In an illustration, the region appears denser and thicker as bony tissue surrounds all fragments, gradually turning the shattered area into a unified structure.
Remodeling Phase — Over months to years, the bone slowly reshapes itself, smoothing excess callus and reorganizing collagen fibers to match the femur’s original architecture. With time, the repaired region regains strength close to pre-injury levels, and on a vector depiction the fracture line gradually fades as uniform bone texture returns.
Because the injury is so destabilizing, rehabilitation plays a crucial role and begins early under controlled supervision. Healing of a comminuted fracture demands careful progression from non–weight-bearing to partial and finally full weight bearing as bone strength returns. Physical therapy restores range of motion at the hip and knee, prevents muscle atrophy, and retrains gait mechanics. A vector illustration of the rehabilitation sequence — beginning with walking aids such as crutches, then advancing to weight-supported treadmill work and strength training — emphasizes that recovery involves more than bone regrowth.
Nutrition and metabolic support are also significant factors. Adequate calcium and vitamin D enable callus mineralization, while protein provides the building blocks for collagen repair. In older adults or individuals with low bone density, bone-strengthening medications or supplemental nutrients may be required to improve healing efficiency. Some vector diagrams show arrows connecting bone, nutrients, and the callus region to demonstrate that healing does not occur in isolation but depends on whole-body health.
The risk of complications is higher with comminuted femur fractures than with simpler fracture patterns, and illustration can help explain why. Possible complications include delayed union, nonunion, malunion (healing in the wrong alignment), infection, blood clots, and long-term gait problems. Educational visuals help patients understand the importance of adherence to follow-up appointments, imaging, and physiotherapy — especially when they see how the fracture requires months of internal biological restructuring even after the visible wound heals.
In its full educational purpose, a vector illustration of a comminuted fracture of the femur showing multiple fragments and orthopedic healing tells a complete story: the moment of catastrophic bone disruption, the surgical methods that restore alignment and stability, the biological phases of bone regeneration, and the gradual return to mobility through rehabilitation. It reinforces that the femur — although extraordinarily strong — is not invincible, and once severely fractured, it demands precise medical intervention, time, and disciplined care to regain full function. By making complex internal events visible, the illustration becomes a guide to understanding both the severity of the injury and the hope that recovery brings through modern orthopedic science and the body’s remarkable capacity to repair itself.