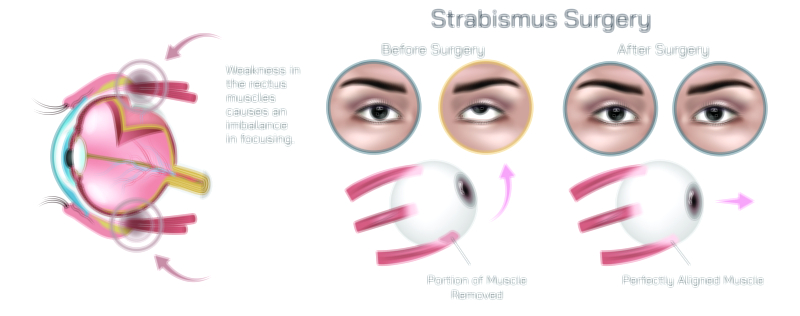
Strabismus for Eye Disease: Showing Misaligned Eyes, Symptoms, and Corrective Treatment
Strabismus is a complex visual disorder in which the two eyes fail to align properly and do not work together to focus on the same visual target. While one eye looks directly at the object being viewed, the other eye may deviate inward, outward, upward, or downward, creating a persistent imbalance in ocular coordination. This misalignment is much more than a cosmetic concern; it interferes with the brain’s ability to combine images from both eyes into a single, unified perception. For children, this condition can disrupt normal visual development, leading to long-term complications if it is not addressed early. For adults, it can cause double vision, impaired depth perception, and significant visual discomfort. Illustrations that depict strabismus for educational purposes often highlight the misaligned visual axes of the two eyes, the neurological consequences of this lack of alignment, the common symptoms that patients experience, and the range of corrective treatments available. These visual materials are designed to clearly portray not only the external appearance of misaligned eyes, but also the internal sensory processes affected by the disorder.
The misalignment seen in strabismus may be constant or intermittent and may happen in one eye or alternate between both. The direction of deviation determines the clinical classification: when an eye turns inward toward the nose, it is called esotropia; when it turns outward away from the nose, it is called exotropia; when it turns upward, it is referred to as hypertropia; and when it turns downward, it is known as hypotropia. Although strabismus often begins in childhood, it can occur at any age, triggered by refractive errors, neurological disorders, trauma, muscle weakness, systemic illness, or eye surgery. In children, the brain attempts to avoid the confusion of receiving two different visual images by suppressing the input from the turned eye. While this adaptation reduces immediate discomfort, it has serious long-term consequences because the suppressed eye does not learn to see effectively. This can lead to amblyopia, a developmental condition in which the vision from the misaligned eye remains permanently weak even though the eye itself may be structurally healthy. A visual explanation of strabismus therefore often shows the dual pathways of what the eyes see versus what the brain processes, reinforcing the idea that visual function depends on neurological development as much as on ocular anatomy.
Adults, however, do not share the same adaptive neurological plasticity as young children. Because their brains are fully developed and cannot suppress the deviated eye as easily, strabismus in adulthood frequently results in double vision. The conflicting images from each eye compete for neural recognition, causing visual confusion and difficulty focusing. This leads to many of the classic symptoms associated with strabismus: blurry vision, unstable eye contact, strained eye movements, impaired depth perception, headaches, difficulty reading for long periods, and awkward posture—such as tilting the head—to try aligning the eyes in a way that temporarily reduces double vision. Educational diagrams that demonstrate these symptoms help viewers understand how strabismus is not merely a matter of eye appearance but a significant cause of functional disability, affecting daily tasks such as driving, sports, academic reading, computer work, and interpersonal communication. For children, the consequences extend beyond visual function; strabismus can affect psychosocial development, self-confidence, and classroom performance. Illustrations of strabismus symptoms therefore include both anatomical and experiential visuals to convey the full impact of the disease.
Diagnosis of strabismus relies on clinical examination, ocular motility testing, and visual acuity assessment. A common evaluation technique involves following the reflection of light on the corneal surface to identify deviation patterns, while another technique uses cover–uncover testing to detect whether the eyes move to maintain fixation. Illustrations that show how each eye responds under cover testing reveal the underlying muscle imbalance that the untrained eye might not recognize. Such visual educational tools are particularly helpful in teaching students and caregivers how clinicians determine which muscles are overacting, underacting, or restricted.
Corrective treatment for strabismus depends on the cause, severity, and age of the patient. One of the most important facts educators emphasize is that treatment must pursue both cosmetic alignment and functional binocular vision, because achieving alignment alone does not guarantee that the brain will use both eyes together properly. For some patients—especially young children—glasses may correct misalignment caused by untreated refractive errors. Hyperopia (farsightedness) can trigger esotropia because the brain strains to focus, causing the eyes to turn inward. Correct prescription lenses help relax the focusing effort and restore alignment. In children with amblyopia associated with strabismus, therapies such as patching the dominant eye or using atropine drops help strengthen the weaker eye by forcing the brain to engage it. This neurological reinforcement is especially effective during early childhood, when the brain is still developing visual pathways.
When misalignment persists despite corrective lenses or when muscle imbalance is structural rather than refractive, treatment focuses on the extraocular muscles—the muscles that move the eyes. Strabismus surgery aims to weaken or strengthen specific muscles to restore balanced eye movement, allowing the eyes to align and work together. Educational illustrations often depict how the surgeon repositions, shortens, or adjusts muscles using techniques such as recession (loosening an overly strong muscle), resection (strengthening a weak muscle), or plication (folding the muscle to increase its pull). Adjustable sutures may be shown as well, allowing post-operative fine-tuning of alignment to ensure the best binocular result. These visuals are crucial for helping students and parents visualize how surgical changes in muscle tension translate into improved eye alignment and visual coordination. For adults with diplopia, therapy often combines surgery with vision training to help the brain relearn binocular fusion.
Non-surgical vision therapy may also play a role, particularly in patients with intermittent deviations or mild binocular dysfunction. Exercises that strengthen convergence, improve accommodation, or enhance visual integration are especially useful in cases of exotropia and convergence insufficiency. Illustrations designed to explain this therapy often depict the difference between misaligned visual axes before treatment and converged visual axes after repeated neuromuscular training. While vision therapy does not replace surgery for most large-angle strabismus cases, it can enhance long-term outcomes by stabilizing binocular control and reducing recurrence.
Understanding strabismus also requires acknowledging the emotional and psychosocial dimensions of the disorder. Children with visible misalignment may experience social challenges, while adults may struggle with self-image, loss of confidence, or social anxiety due to noticeable deviation or unstable eye contact. Corrective treatment can therefore improve both visual function and emotional well-being. Educational materials featuring strabismus illustrations help normalize the disorder, encourage families to seek early evaluation, and reinforce the hopeful message that treatment is highly effective when pursued in a timely and consistent manner.
A complete vector illustration of strabismus does more than show eyes pointing in different directions. It tells a comprehensive story: how misalignment arises, how the brain responds to conflicting visual signals, how symptoms appear in real-world experiences, and how corrective treatments—from glasses to therapy to surgery—work to restore alignment and binocular harmony. By presenting strabismus through clear visual language rather than complex terminology alone, such educational graphics enhance understanding for clinicians, trainees, patients, teachers, and families. They deepen awareness of a condition that is often underestimated and highlight the importance of timely intervention to protect visual development, daily comfort, and lifelong visual health.