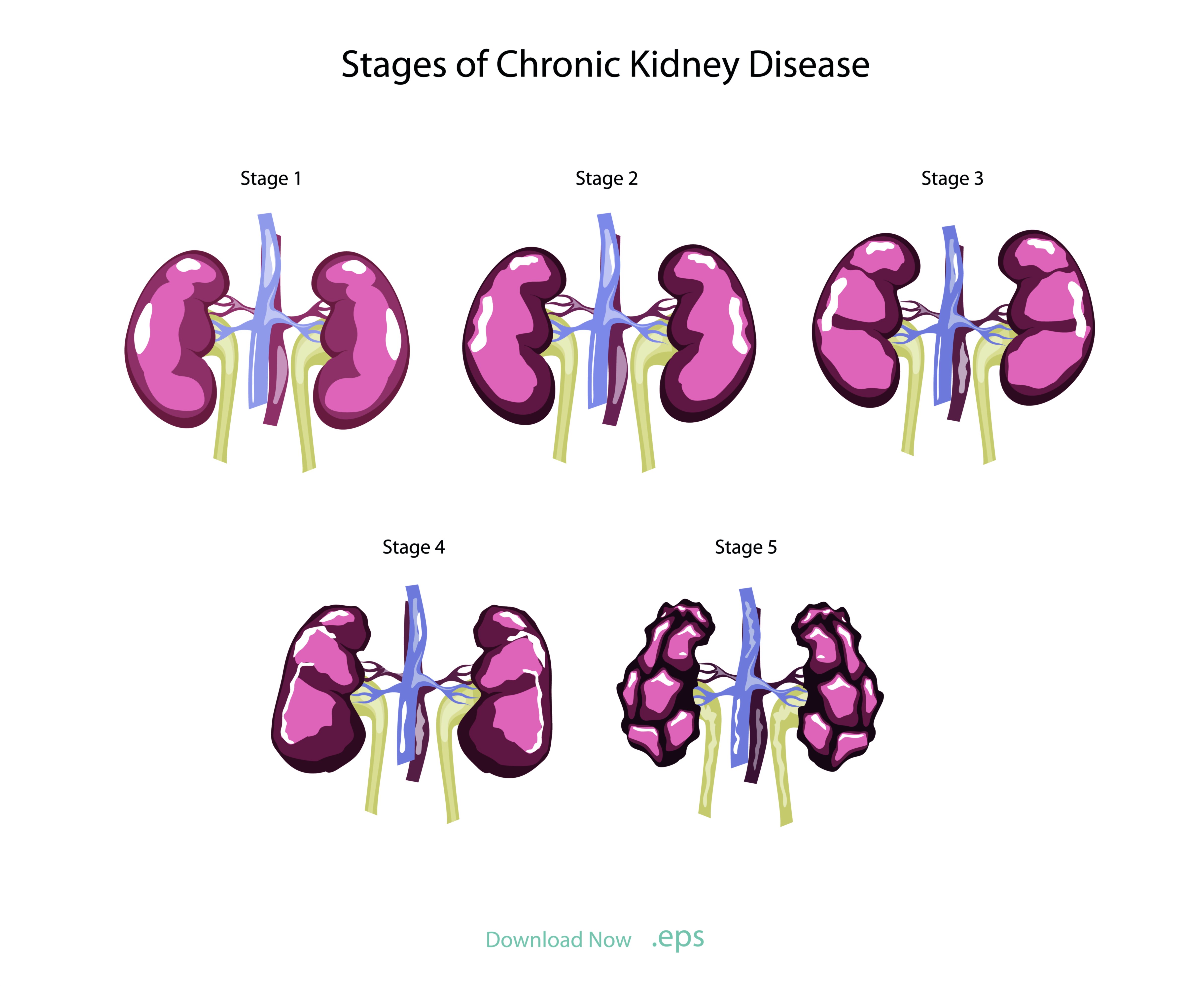
Stages of Chronic Kidney Disease — Progressive Decline of Renal Function
Chronic kidney disease progresses through a series of clearly defined stages that reflect gradual loss of filtration ability and increasing structural damage to kidney tissue. These stages, classified based on the glomerular filtration rate, are not merely labels but markers of physiological decline that predict how the body will respond to accumulating waste products, fluid imbalance, and changes in blood chemistry. While chronic kidney disease unfolds slowly and silently in its earliest phase, each subsequent stage introduces more noticeable systemic effects. The journey from stage 1 to stage 5 demonstrates how an organ that supports homeostasis across the entire body gradually loses the ability to clear wastes, balance electrolytes, regulate blood pressure, produce hormones, and maintain fluid distribution. Understanding these stages is vital because early intervention, lifestyle management, and medical therapy can slow progression dramatically, while late-stage damage demands complex replacement treatments such as dialysis or transplantation.
Stage 1 chronic kidney disease represents the earliest phase, where kidney function remains nearly normal from a filtration standpoint but underlying biological or structural damage has already begun. Often at this point the glomerular filtration rate remains above ninety milliliters per minute, yet microscopic signs exist—such as protein or blood in the urine—that indicate nephron stress. In many cases the patient feels entirely normal because the kidneys still possess a large functional reserve. However, signs of vulnerability already appear, especially in the presence of diabetes, high blood pressure, autoimmune disease, or inherited renal disorders. This early stage emphasizes the deceptive nature of chronic kidney disease because the body masks symptoms through compensatory mechanisms. Early identification depends not on symptoms but on screening tests that detect subtle abnormalities, and early management targets the root cause to prevent further damage before significant nephron loss occurs.
In stage 2, kidney function shows a mild decline as the filtration rate falls between sixty and eighty-nine milliliters per minute. Even here symptoms are often absent or minimal, which means many patients still do not realize they are losing renal capacity. Despite this near-silent phase, harmful processes take shape: blood vessel damage, inflammatory responses, oxidative stress in nephrons, and hormonal changes that start influencing blood pressure and protein metabolism. Protein leakage in urine often becomes more persistent, signaling ongoing glomerular injury. Although everyday life may remain unaffected, this stage represents a crucial turning point because intervention can reduce workload on nephrons and significantly slow progression through later stages. Blood pressure control, glucose regulation, sodium limitation, smoking cessation, moderate protein intake, and weight management are especially important during this period because they directly influence the rate of kidney tissue decline.
Stage 3 defines the midpoint of chronic kidney disease and marks the point at which metabolic changes begin to manifest more visibly. The glomerular filtration rate declines to between thirty and fifty-nine milliliters per minute, meaning the kidneys can no longer fully handle their filtering responsibilities. Stage 3 is often divided into early and late segments because the metabolic burden increases noticeably as filtration declines. Waste products such as urea and creatinine begin accumulating in the bloodstream, leading to fatigue, difficulty concentrating, swelling in the legs or around the eyes, nighttime urination, and appetite reduction. As erythropoietin production decreases, anemia becomes a common symptom and contributes to weakness and cold intolerance. Mineral balance begins shifting as vitamin D activation drops, leading to rising phosphorus levels and declining calcium absorption. These changes lay the foundation for bone mineral disorders over time. At this stage, medical management becomes more intensive. Physicians work to stabilize blood pressure, control blood sugar, manage electrolyte disturbances, treat anemia, protect heart health, and prevent metabolic acidosis. Stage 3 often marks the first time many patients realize their kidney disease is not temporary but progressive.
Stage 4 marks severe kidney impairment, where filtration falls to between fifteen and twenty-nine milliliters per minute. At this point, the body struggles to maintain chemical equilibrium, and symptoms intensify. Excess fluid may accumulate, causing swelling, breathlessness, or hypertension as the vascular system retains more volume than it can regulate. Uremic toxins accumulate to higher levels, increasing nausea, metallic taste, sleep disruption, reduced appetite, and cognitive fatigue. Bone disease becomes more pronounced as calcium balance destabilizes and phosphorus remains elevated. High potassium levels in the bloodstream become particularly dangerous because they threaten heart rhythm stability. Stage 4 also marks the phase where care transitions from lifestyle-focused preservation of kidney function toward planning for renal replacement therapy. The healthcare team prepares patients for vascular access creation for dialysis, education about dialysis options, and evaluation for kidney transplantation. Although this stage is difficult, medical therapy can still slow or stabilize progression and delay kidney failure if treatment is consistent and metabolic stress is minimized.
Stage 5 represents end-stage renal disease, in which the filtration rate falls below fifteen milliliters per minute and the kidneys can no longer sustain life without external assistance. At this point, most nephrons are nonfunctional, and no amount of compensation remains to offset the accumulation of toxic metabolic waste. The systemic effects of kidney failure intensify sharply: fluid builds up in the lungs, heart function deteriorates, potassium levels threaten cardiac arrest, severe anemia reduces oxygenation, bone loss accelerates, blood pressure becomes difficult to control, and uremic toxins begin to affect neurological function. The body enters a crisis state because internal chemistry cannot be regulated naturally. Dialysis becomes necessary to remove waste and fluid artificially, either through hemodialysis in a clinic or peritoneal dialysis at home. For eligible patients, kidney transplantation provides the best long-term outcome, restoring renal function far more completely than dialysis and improving daily quality of life. Without dialysis or transplant, stage 5 kidney failure becomes fatal. Although this represents the final clinical stage, care continues to focus on symptom relief, emotional support, dietary regulation, and medical stability.
The movement from stage 1 to stage 5 is not simply a linear decline but a reflection of the kidney’s shrinking resilience. In the early stages, remaining nephrons compensate successfully, hiding the underlying damage. As compensation fails, symptoms expand from biochemical abnormalities to visible systemic effects. Each stage amplifies the risk of cardiovascular disease, metabolic disorder, infection vulnerability, bone disease, and neurological complications. Chronic kidney disease therefore becomes a condition not confined to the renal system but one that influences nearly every organ through disrupted homeostasis.
A core feature of chronic kidney disease progression is that early detection can dramatically alter the future course of illness. When identified and treated at stages 1 or 2, kidney decline often slows to a degree that prevents the need for dialysis or transplant for many years. At stage 3, treatment remains effective at preserving remaining function and preventing complications. Once patients reach stage 4 and 5, personal and medical demands increase sharply, requiring complex treatment plans, strict dietary steps, and long-term therapy. Whether a patient progresses quickly or slowly depends on many variables: blood pressure control, blood sugar stability in diabetes, smoking status, dietary salt intake, obesity, genetic predisposition, autoimmune activity, and exposure to nephrotoxic medications or chemicals.
The five stages of chronic kidney disease therefore provide a roadmap not only for diagnosis and treatment but also for education, empowerment, and prevention. Each transition between stages signals a shift in risks, responsibilities, treatment goals, and medical priorities. From the silent beginning of structural damage to the life-altering reality of renal failure, chronic kidney disease represents a progression that can dramatically influence an individual physically, emotionally, socially, and economically. Yet that same progression provides a clear opportunity for early detection, consistent monitoring, and proactive lifestyle adjustment that may delay its advance and protect quality of life. Understanding the stages allows individuals, caregivers, and clinicians to recognize the signs earlier, intervene effectively, and support long-term health despite the progressive nature of kidney disease.