Pantoprazole Medication – Comprehensive Educational Summary on Mechanism of Action, Gastric Acid Control, Proton Pump Inhibition, Clinical Uses, Dosage Considerations, Side Effects, Precautions, and Therapeutic Role in Digestive Health
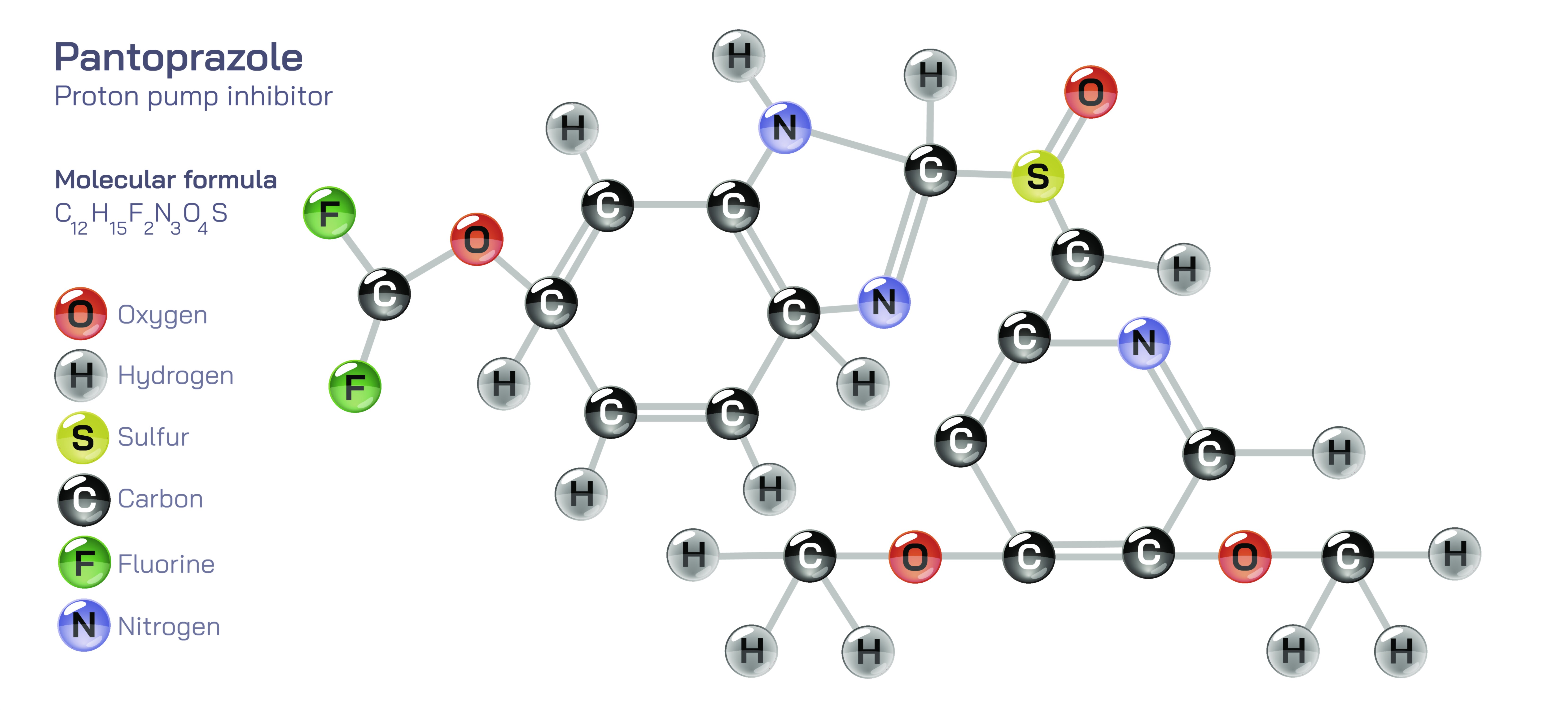
Pantoprazole is a widely prescribed gastrointestinal medication belonging to the drug class known as proton pump inhibitors (PPIs), and it has become one of the most important therapeutic tools in modern medicine for managing disorders caused by excess stomach acid. While its effects are most noticeable within the digestive system, pantoprazole works through a deep biochemical mechanism that targets the molecular machinery of acid production rather than simply neutralizing acid after it forms. This strategic approach allows it to provide long-lasting relief from burning pain, ulcer discomfort, acid reflux irritation, and other complications associated with hyperacidity. Its clinical value lies in its ability not only to reduce symptoms but also to promote healing in the esophagus, stomach, and duodenum by maintaining an internal environment in which damaged tissues can recover.
Pantoprazole works by inhibiting the gastric proton pump, the final and most important enzyme responsible for releasing acid into the stomach. Inside the stomach, specialized cells called parietal cells pump hydrogen ions into the stomach cavity using the H⁺/K⁺ ATPase pump, generating highly acidic conditions needed for digestion. In conditions such as gastroesophageal reflux disease (GERD), peptic ulcer disease, Zollinger–Ellison syndrome, or chronic gastritis, the stomach produces far more acid than necessary, causing inflammation, discomfort, and tissue damage. Pantoprazole is designed to bind irreversibly to the proton pump, keeping it inactive so that fewer hydrogen ions are released. Because the body cannot restart acid production until new proton pumps are synthesized, pantoprazole produces a long-lasting reduction in acidity—an effect far stronger and more sustained than that of antacids or H2-receptor blockers. This prolonged control enables healing of ulcers and erosions, reduces heartburn and regurgitation episodes, protects the esophagus from acid injury, and decreases the risk of gastrointestinal bleeding.
Clinically, pantoprazole is widely used for GERD (gastroesophageal reflux disease), one of the most common digestive disorders where stomach acid flows backward into the esophagus, causing burning pain, throat irritation, cough, and long-term risk of esophageal injury. It is also prescribed for peptic ulcers, whether located in the stomach or duodenum, because lowering acidity allows ulcer surfaces to regenerate. In addition, pantoprazole is valuable for preventing and treating ulcers caused by long-term nonsteroidal anti-inflammatory drug (NSAID) use, which weakens the stomach lining and increases susceptibility to acid erosion. In more rare but severe disorders such as Zollinger–Ellison syndrome, where tumors cause extreme acid secretion, pantoprazole becomes a vital long-term therapy for protecting digestive tissues from ulceration. Physicians also use pantoprazole as part of triple or quadruple therapy for H. pylori infection, where suppressing acid enhances antibiotic effectiveness and supports mucosal repair. These broad therapeutic roles illustrate how a single molecular pathway—acid suppression—can improve multiple digestive health outcomes when controlled safely and effectively.
Pantoprazole is commonly available as tablets, delayed-release capsules, and intravenous injections. Oral tablets are often taken once daily before breakfast because food activates proton pumps, and pantoprazole binds most effectively when these pumps are active. The medication’s delayed-release formulation protects it from breakdown in stomach acid, ensuring it reaches the intestine before absorption into the bloodstream. The dosage varies depending on the condition, severity of symptoms, and treatment goals. Short-term use may be sufficient for transient reflux or mild ulcers, while chronic GERD or hypersecretory disorders may require long-term therapy under medical supervision. Intravenous formulations are reserved for hospitalized patients with severe ulcers, gastrointestinal bleeding risk, or inability to take oral medication.
Like all effective medications, pantoprazole must be used carefully to maximize benefits while minimizing potential risks. Short-term side effects are usually mild and may include headache, nausea, diarrhea, abdominal discomfort, or dizziness, though many individuals tolerate the medication without noticeable effects. Long-term use has special considerations because sustained suppression of stomach acid alters the digestive environment. Stomach acid plays a role not only in food digestion but also in nutrient absorption and pathogen defense, so prolonged acid reduction may decrease the absorption of vitamin B12, calcium, magnesium, and iron, potentially increasing the risk of deficiencies or weak bone density in susceptible individuals. Altered acidity can also influence gut microbiota and may increase vulnerability to infections such as Clostridioides difficile in certain patients. These risks do not diminish the value of pantoprazole; instead, they underscore the importance of medical supervision during extended therapy to ensure that the medication is used with precision rather than indiscriminately.
There are also precautions for specific populations. Pregnant or breastfeeding individuals should consult a physician before using pantoprazole to weigh benefits against potential risks. People with severe liver disease may require adjusted dosing. Pantoprazole should not be stopped abruptly after long-term use without medical guidance, because sudden withdrawal may trigger rebound acid hypersecretion, worsening symptoms temporarily. When discontinuation is advised, tapering dosage gradually allows proton pump activity to normalize without dramatic fluctuations.
Educationally, pantoprazole offers valuable insight into how targeted biochemical intervention can resolve disorders rooted in everyday physiology. It teaches that disease does not always result from infection or structural damage but sometimes from excessive activity of a normal bodily process, such as acid secretion. It reveals how molecular pharmacology can selectively block a tiny protein pump and, through that mechanism, relieve pain, reduce inflammation, heal tissues, and restore quality of life. It demonstrates why digestive health relies not only on dietary habits but on chemical regulation inside the stomach and duodenum.
Ultimately, pantoprazole is more than a medication for heartburn—it is a highly engineered tool that protects the digestive tract from acid-induced injury, promotes deep healing of ulcers, and safeguards the esophagus from chronic damage caused by reflux. When used responsibly and under guidance, it allows patients to regain comfort, nutrition, and digestive stability, preserving both immediate well-being and long-term gastrointestinal health.