Osteoarthritis vs Rheumatoid Arthritis: Joint Damage and Inflammation Differences Explained
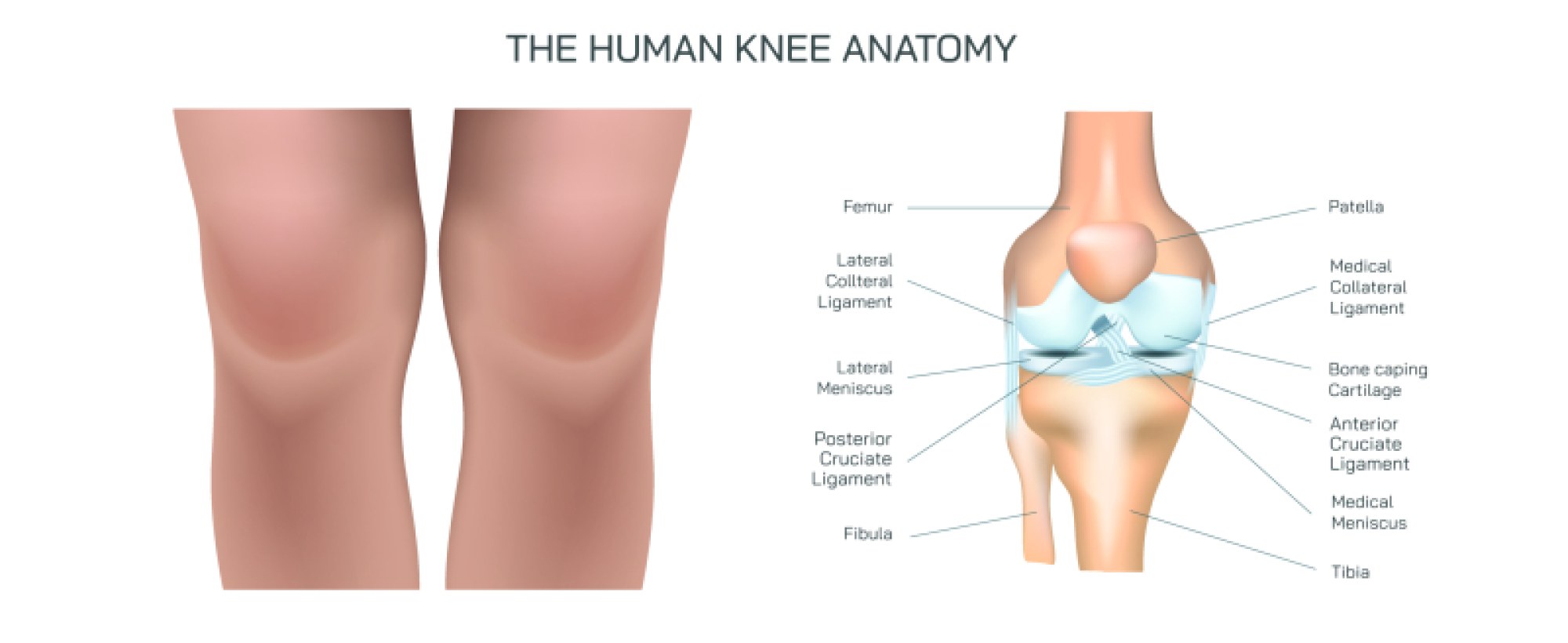
Osteoarthritis and rheumatoid arthritis are two of the most common joint disorders, but they differ fundamentally in their origins, progression, and the way they damage joint structures. Although both conditions cause pain, stiffness, and declining mobility, their mechanisms are not the same, and understanding their differences requires looking closely at the tissues involved in inflammation and destruction inside affected joints. Osteoarthritis is primarily a degenerative disorder in which the protective cartilage that cushions the ends of bones gradually wears away due to mechanical stress, aging, metabolic factors, or prior trauma. Rheumatoid arthritis, in contrast, is an autoimmune disease in which the immune system mistakenly attacks the synovial lining of the joints, triggering persistent inflammation that destroys cartilage, bone, ligaments, and surrounding tissues. When these two conditions are viewed side by side, a clearer picture emerges: osteoarthritis represents the gradual breakdown of joint mechanics, whereas rheumatoid arthritis reflects a systemic immune-driven process that progressively inflames and erodes joints.
In osteoarthritis, the earliest changes occur in the articular cartilage, a smooth and resilient tissue that enables frictionless motion between bones. Over decades of wear, repetitive movement, or excess body weight, cartilage loses its elasticity, becomes dehydrated, and begins to fray. Because cartilage contains no blood vessels and cannot regenerate effectively, once this breakdown begins it accelerates slowly but inevitably. As cartilage thins, the underlying bone is exposed and starts to remodel itself in response to abnormal pressure. This leads to the formation of hard bony enlargements at the joint margins known as osteophytes, which contribute to stiffness and reduced motion. Beneath the surface, the subchondral bone becomes denser and may develop microscopic fractures or cysts. Although osteoarthritis can include mild inflammation, this inflammation is secondary to mechanical wear and is not the primary driving force of the disease. The overall result is pain triggered by joint use, loss of cushioning, grinding or creaking sensations during movement, and a gradual worsening over many years.
Rheumatoid arthritis begins in a completely different way. Instead of mechanical wear, it is driven by a malfunction of the immune system. The body produces autoantibodies that target the synovial membrane, the delicate tissue that lines each joint and produces lubricating fluid. This immune attack transforms the synovial lining into an inflamed, thickened mass called pannus, which invades the joint space much like an overgrown tissue. Pannus releases inflammatory chemicals that break down cartilage and bone while also causing swelling and pain. Unlike osteoarthritis, pain in rheumatoid arthritis is often most intense after periods of inactivity, such as in the morning, because inflammation peaks during rest rather than activity. Over time, the chronic immune response leads to weakening of tendons and ligaments that stabilize the joint. Without support, bones shift out of position, causing deformities and instability that can become irreversible if the disease is not treated aggressively.
Another major difference between these conditions lies in their distribution across the body. Osteoarthritis typically affects weight-bearing or heavily used joints, such as knees, hips, spine, and the small joints at the base of the thumb. It is often asymmetrical, affecting only one or a few joints depending on lifestyle, occupation, injury history, and age. In contrast, rheumatoid arthritis almost always affects multiple joints in a symmetrical pattern, such as both wrists, both ankles, or the same small finger joints on both hands. This symmetry is a hallmark of autoimmune involvement and highlights that rheumatoid arthritis is a systemic disease that can affect organs outside the joints, including the heart, lungs, and eyes through chronic inflammation. Fatigue, low-grade fever, anemia, and weight loss often accompany rheumatoid arthritis because inflammation affects the entire body, not just the joint spaces.
When comparing pain patterns between the two conditions, the contrast becomes even clearer. In osteoarthritis, pain typically worsens with movement and improves with rest because mechanical stress directly aggravates joint surfaces. People with osteoarthritis often describe difficulty climbing stairs, walking long distances, or gripping objects tightly due to pressure on damaged joints. In rheumatoid arthritis, resting or inactivity may increase stiffness and pain, while gentle motion can provide relief by dispersing inflammatory fluid and improving circulation. Morning stiffness is brief in osteoarthritis but prolonged in rheumatoid arthritis, sometimes lasting an hour or more. These differences in timing reflect the distinction between wear-and-tear damage and immune-driven inflammation.
Under medical imaging, the contrast between osteoarthritis and rheumatoid arthritis becomes even more dramatic. X-rays of osteoarthritis show narrowing of joint space, sclerosis of subchondral bone, and osteophyte formation. In rheumatoid arthritis, imaging demonstrates erosion of bone at the edges of joints where pannus tissue has been attacking bone surfaces. The surrounding soft tissues may appear swollen, and advanced cases show joint deformities caused by ligament weakening. Even in early disease, ultrasound or MRI can reveal active synovitis in rheumatoid arthritis long before structural damage occurs. These tools highlight the predictable degenerative pattern of osteoarthritis and the aggressive, immune-mediated destruction of rheumatoid arthritis.
In terms of progression, osteoarthritis tends to worsen gradually and mainly affects mobility and comfort rather than general health. Rheumatoid arthritis, however, can advance rapidly and without treatment may lead to disability within a few years. The modern treatment landscape reflects this difference. Management of osteoarthritis focuses on weight control, physical therapy, pain relief, improved biomechanics, and sometimes joint replacement. Treatment of rheumatoid arthritis targets the immune system using disease-modifying antirheumatic drugs and biologic therapies designed to stop inflammation before it causes permanent damage. Early diagnosis is critical because joint destruction in rheumatoid arthritis can be halted or slowed dramatically with timely intervention.
Despite their differences, both forms of arthritis demonstrate how essential healthy joints are for independence, mobility, and quality of life. Osteoarthritis shows how mechanical strain and time slowly reshape joint structures, while rheumatoid arthritis reveals how a misdirected immune system can attack the very tissues it is meant to protect. The experience of pain and stiffness links the two conditions, but the processes inside the joints tell two distinct stories: one of physical wear and degeneration, the other of autoimmunity and chronic inflammation. Understanding the contrast between the two is crucial not only for accurate diagnosis and treatment but also for helping those affected recognize why their symptoms behave the way they do. When viewed together, osteoarthritis and rheumatoid arthritis illustrate the depth and complexity of joint biology and the many factors required to maintain smooth and pain-free movement throughout life.