Types of Surgical Stitches — Techniques and Wound Closure Methods Explained
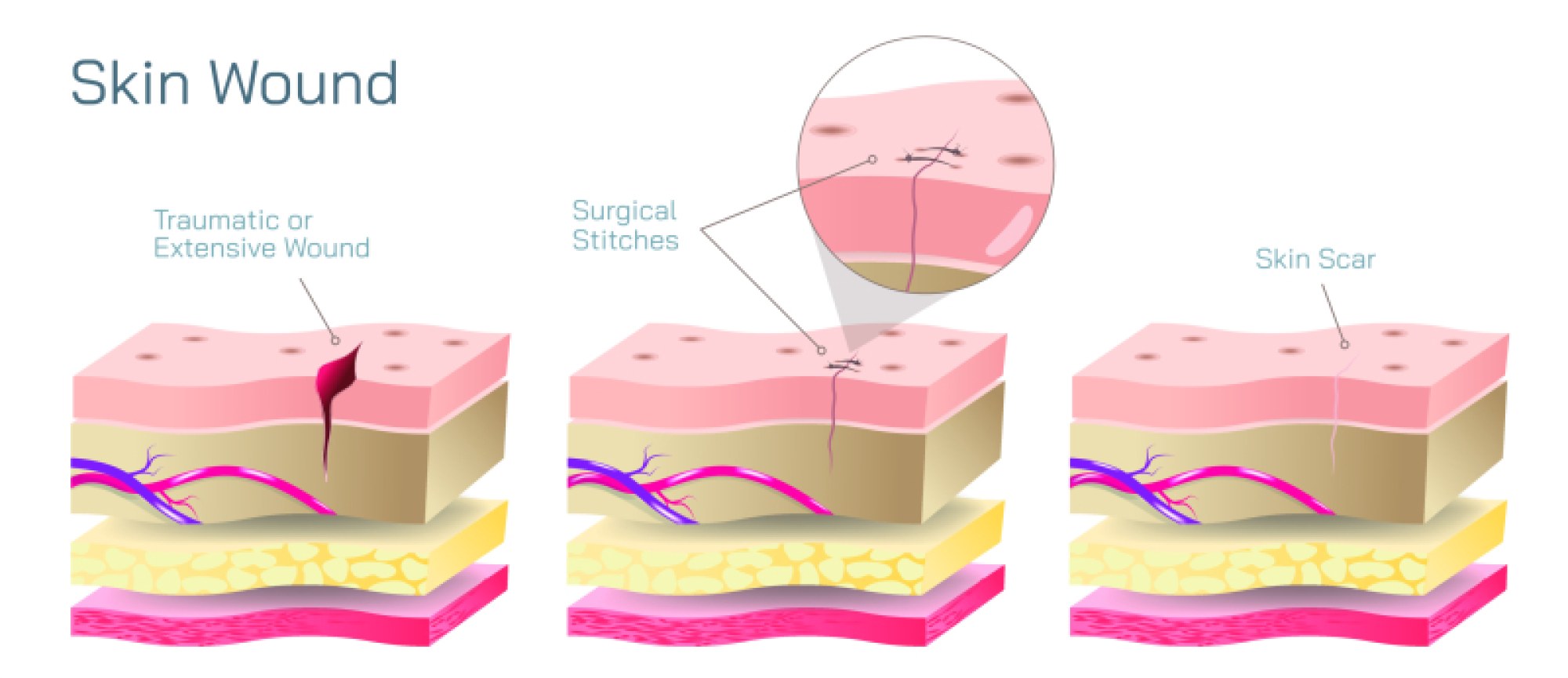
Surgical stitches, also known as sutures, represent one of the oldest and most fundamental practices in medicine, yet they remain a cornerstone of modern surgery because they serve a purpose that is both mechanical and biological: closing wounds so that the body can heal in the safest, cleanest, and most structurally stable manner possible. Whether the injury is caused by trauma or is the result of an intentional surgical incision, the body requires a structured environment to regenerate tissue without infection, bleeding, or reopening of the wound. Sutures achieve this by bringing wound edges together, reducing stress on the injured surface, and maintaining alignment of underlying tissues long enough for healing to take place. Although the act of stitching a wound may appear simple from the outside, the selection of suture type and technique is a sophisticated clinical decision based on the location of the wound, thickness and sensitivity of surrounding tissues, degree of tension, risk of infection, cosmetic considerations, and expected healing time. These factors determine why surgeons must choose different suture materials and stitching patterns for different regions of the body, and why mastering wound closure is as much an art of precision as it is a science of tissue mechanics and healing physiology.
Sutures can be broadly categorized by their composition, the most fundamental distinction being absorbable versus non-absorbable sutures. Absorbable sutures are designed to break down naturally inside the body through enzymatic or hydrolytic processes over a defined period, removing the need for later removal. They are primarily used in internal tissues, deep muscle layers, and organs where long-term support is required only during the initial healing phase. Common absorbable suture materials include polyglycolic acid, polydioxanone, and catgut derived from purified collagen. These sutures offer the advantage of disappearing once they have completed their job, reducing discomfort and simplifying postoperative care. In contrast, non-absorbable sutures, made from materials such as nylon, polypropylene, silk, or stainless steel, do not degrade over time and provide permanent support. They are used when tissues require long-lasting mechanical strength or where healing is slow, such as in skin closure, vascular procedures, or orthopedic surgeries. These sutures remain in place indefinitely unless they are removed manually, allowing continued reinforcement in anatomically demanding regions.
Just as material determines longevity, structure of the thread plays an important role in wound behavior. Sutures can be monofilament or multifilament (braided). Monofilament sutures consist of a single smooth strand that glides easily through tissue and minimizes microbial adherence, making them beneficial for contaminated wounds or those at higher risk of infection. Their smoothness reduces friction, but they may be more difficult to handle because they possess less knot security and stiffness. Braided sutures, on the other hand, consist of multiple intertwined filaments that offer superior handling, flexibility, and knot security. Their woven surface grips tissue effectively, but this same property makes them more prone to harboring bacteria, meaning they are generally avoided in wounds that require sterile protection. Understanding these structural differences allows surgeons to balance the competing needs of tissue compatibility, durability, resistance to tearing, and infection control.
Another defining element of surgical stitches involves the pattern of closure, determined not by the material but by the technique used to pass the suture through tissue. One of the most widely used patterns is the simple interrupted stitch, where each stitch is individually placed and tied. This approach offers excellent control over wound tension because each knot functions independently; if one knot fails or becomes infected, the rest of the closure remains secure. It is versatile and suitable for many types of wounds, especially those with uneven edges or variable depth. Another common technique is the continuous (running) suture, where a single thread is passed along the entire wound and tied at both ends. Continuous suturing distributes tension evenly and seals the wound more rapidly, which is particularly valuable in long incisions such as abdominal or obstetric surgeries. However, the weakness of this method lies in its dependence on one thread—if one section breaks or becomes compromised, the entire closure may loosen.
Certain suture techniques serve more specialized purposes. The vertical and horizontal mattress stitches are effective for closing wounds under high tension or for wounds with edges that tend to invert rather than align naturally. These stitches distribute tension across a wider tissue area and promote eversion of the wound edges, which is critical for optimal long-term cosmetic healing because inverted skin edges increase scarring. The subcuticular or intradermal suture is another technique highly valued in cosmetic and plastic surgery because the suture lies beneath the outer surface of the skin and leaves minimal visible marks. It is often paired with absorbable sutures so that removal is unnecessary. For deep wounds that require multi-layer closure, surgeons may combine techniques by closing deeper layers with absorbable sutures before using non-absorbable stitches on the skin surface. Each layer of closure reduces tension on the next, creating stability that supports proper healing.
Beyond traditional sutures, surgeons may employ specialized stitching methods for particular clinical needs. The purse-string suture, for example, is stitched in a circular fashion and tightened like a drawstring, useful for closing circular openings such as those created during intestinal or cardiovascular procedures. The figure-of-eight suture reinforces tissues subjected to significant pressure or bleeding, commonly applied in vascular surgery and orthopedic soft-tissue repair. In tendon and ligament surgeries, heavily specialized suturing patterns such as the Krackow and Bunnell techniques interlock deeply into strong connective tissue to prevent rupture during the healing period. These techniques go beyond closure—they are load-bearing systems that must withstand biomechanical forces without compromising mobility or inducing anatomical dysfunction.
The decision to select one suture method over another is anchored in knowledge of wound physiology and biomechanics. Skin, muscle, fascia, tendons, and internal organs heal at different rates and respond differently to tension. A wound located on the face heals quickly and requires minimal tension closure, making fine sutures and cosmetic techniques appropriate. A wound across the knee or shoulder, however, is constantly exposed to stretching and movement, requiring deep anchoring stitches and layered closure to prevent dehiscence. In contaminated wounds, the surgeon selects materials and patterns that reduce the risk of trapping bacteria, opting for monofilament sutures and interrupted stitching to allow drainage. In clean surgical environments, continuous sutures may maximize healing efficiency. Even cosmetic outcomes depend on technique: inverted or misaligned edges can lead to hypertrophic scars, while properly everted edges and deep tissue approximation minimize scar formation.
In modern medicine, sutures coexist with alternatives such as surgical staples, tissue adhesives, and skin closure strips. Yet these alternatives do not replace sutures—they complement them. Staples are preferred in time-critical surgeries where speed is essential, but they are not suited for delicate or high-precision regions. Adhesives provide excellent cosmetic outcomes for superficial linear wounds but lack strength for deep layers. Sutures remain indispensable because they are adaptable to virtually every tissue type and can be customized for strength, depth, precision, and healing profile. Their continued relevance reflects how the human body heals—not instantaneously, but gradually through biological repair processes that require physical support during recovery.
Ultimately, the science of surgical stitches is more than the mechanical act of sewing tissue. It is a discipline grounded in profound respect for how the human body repairs itself. Every suture placement influences the future of that wound—whether it will heal cleanly or develop infection, whether it will support tissue regeneration or fall apart under stress, whether the scar will fade naturally or remain prominent for life. Surgeons combine an understanding of biomaterials, anatomical forces, immune responses, and tissue dynamics to guide wound closure decisions that support optimal outcomes. The types of stitches and techniques used reflect this integration of engineering, biology, and clinical judgment. When chosen and applied skillfully, sutures become invisible participants in the healing journey, silently holding the body together long enough for nature to complete the work of restoration.